

Optimal Cervical Cancer Screening in Women Vaccinated Against Human Papillomavirus
- PMID: 27754955
- PMCID: PMC5068562
- DOI: 10.1093/jnci/djw216
Optimal Cervical Cancer Screening in Women Vaccinated Against Human Papillomavirus
Abstract
Background: Current US cervical cancer screening guidelines do not differentiate recommendations based on a woman's human papillomavirus (HPV) vaccination status. Changes to cervical cancer screening policies in HPV-vaccinated women should be evaluated.
Methods: We utilized an individual-based mathematical model of HPV and cervical cancer in US women to project the health benefits, costs, and harms associated with screening strategies in women vaccinated with the bivalent, quadrivalent, or nonavalent vaccine. Strategies varied by the primary screening test, including cytology, HPV, and combined cytology and HPV "cotesting"; age of screening initiation and/or switching to a new test; and interval between routine screens. Cost-effectiveness analysis was conducted from the societal perspective to identify screening strategies that would be considered good value for money according to thresholds of $50 000 to $200 000 per quality-adjusted life-year (QALY) gained.
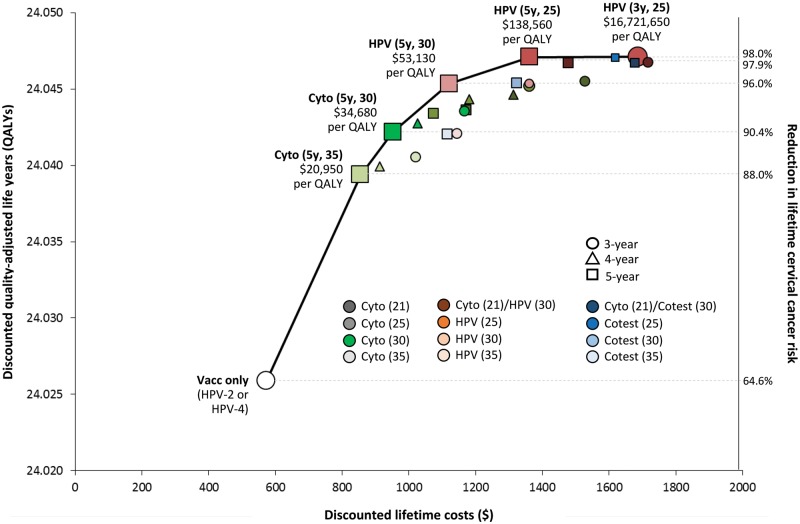
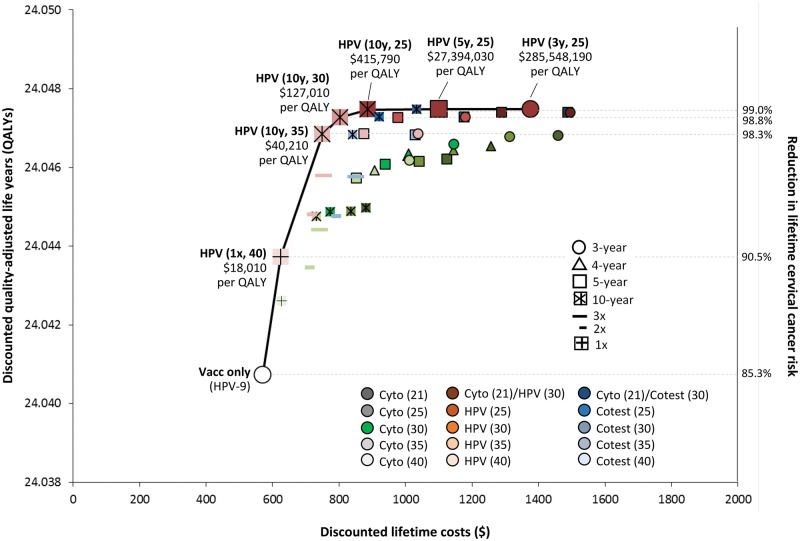
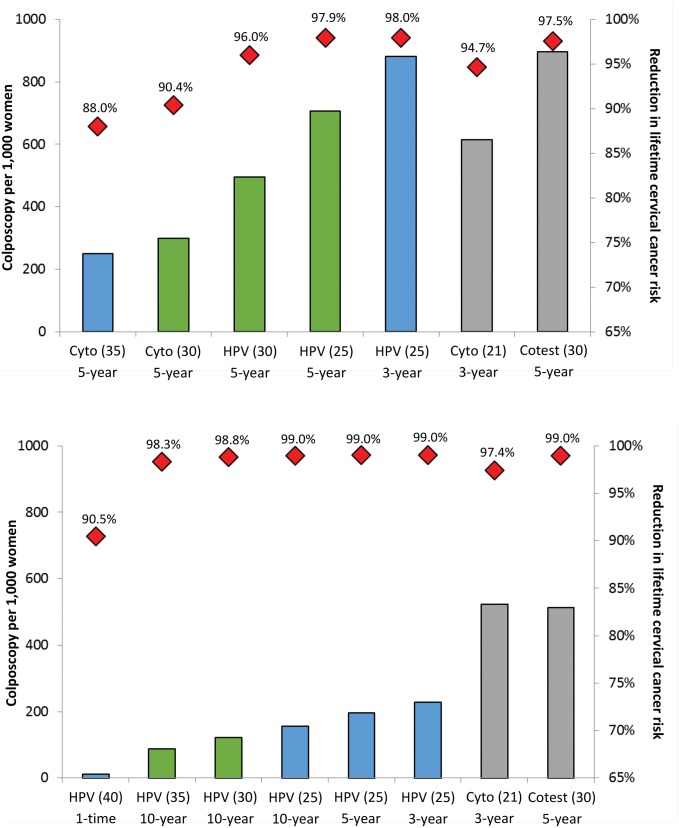
Results: Among women fully vaccinated with the bivalent or quadrivalent vaccine, optimal screening strategies involved either cytology or HPV testing alone every five years starting at age 25 or 30 years, with cost-effectiveness ratios ranging from $34 680 to $138 560 per QALY gained. Screening earlier or more frequently was either not cost-effective or associated with exceedingly high cost-effectiveness ratios. In women vaccinated with the nonavalent vaccine, only primary HPV testing was efficient, involving decreased frequency (ie, every 10 years) starting at either age 35 years ($40 210 per QALY) or age 30 years ($127 010 per QALY); with lower nonavalent vaccine efficacy, 10-year HPV testing starting at earlier ages of 25 or 30 years was optimal. Importantly, current US guidelines for screening were inefficient in HPV-vaccinated women.
Conclusions: This model-based analysis suggests screening can be modified to start at later ages, occur at decreased frequency, and involve primary HPV testing in HPV-vaccinated women, providing more health benefit at lower harms and costs than current screening guidelines.
© The Author 2016. Published by Oxford University Press. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
When Less is More.J Natl Cancer Inst. 2016 Oct 18;109(2):djw240. doi: 10.1093/jnci/djw240. Print 2017 Feb. J Natl Cancer Inst. 2016. PMID: 27756809 No abstract available.
References
-
- Moyer VA. Screening for Cervical Cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;156:880–891. - PubMed
-
- Future II Study Group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. N Engl J Med. 2007;356(19):1915–1927. - PubMed
-
- Paavonen J, Naud P, Salmeron J, et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): Final analysis of a double-blind, randomised study in young women. Lancet. 2009;374(9686):301–314. - PubMed
