

Burden of Severe Respiratory Syncytial Virus Disease Among 33-35 Weeks' Gestational Age Infants Born During Multiple Respiratory Syncytial Virus Seasons
- PMID: 27755464
- PMCID: PMC5242218
- DOI: 10.1097/INF.0000000000001377
Burden of Severe Respiratory Syncytial Virus Disease Among 33-35 Weeks' Gestational Age Infants Born During Multiple Respiratory Syncytial Virus Seasons
Abstract
Background: Moderate-late preterm infants, 33-35 weeks' gestational age (wGA), are at increased risk for respiratory syncytial virus hospitalization (RSVH). The objective of this study is to quantify the burden of RSVH in moderate-late preterm infants.
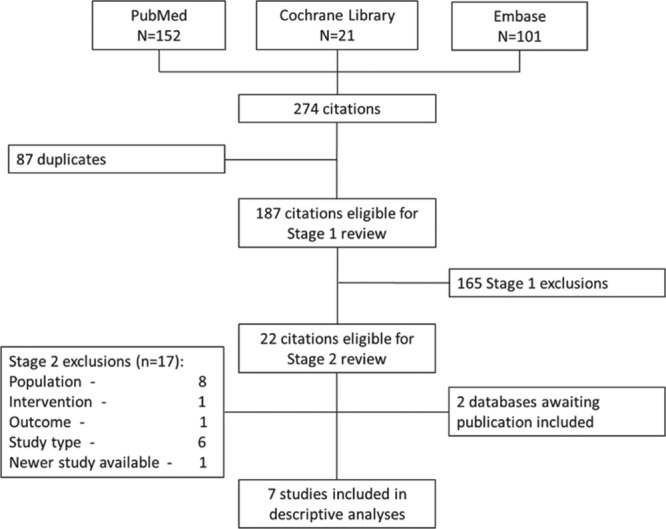
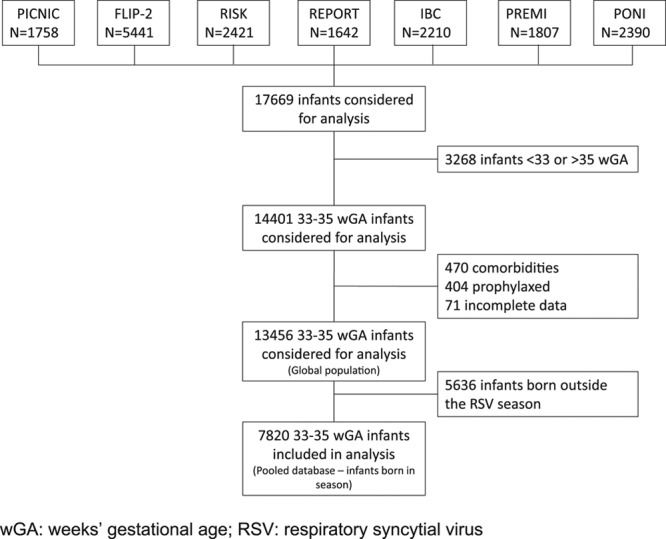
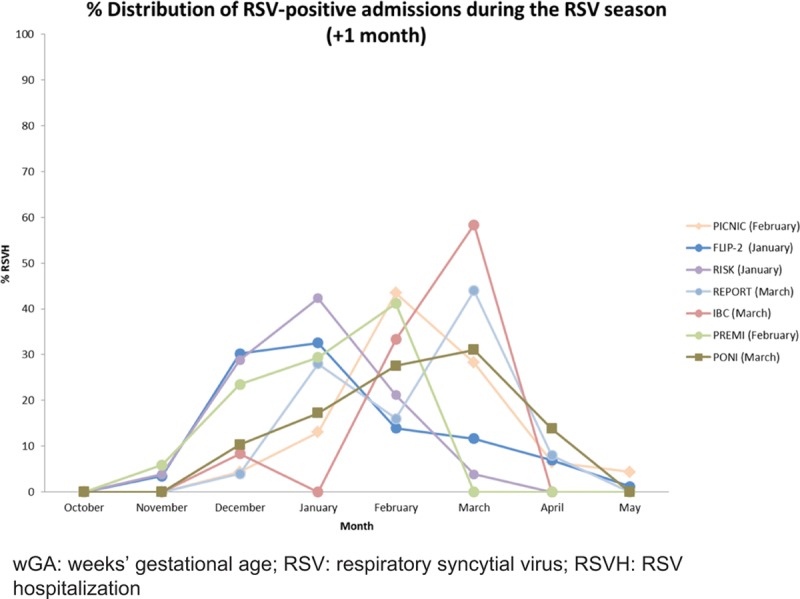
Methods: A pooled analysis was conducted on RSVH from 7 prospective, observational studies in the Northern Hemisphere from 2000 to 2014. Infants' 33-35 wGA without comorbidity born during the respiratory syncytial virus season who did not receive respiratory syncytial virus immunoprophylaxis were enrolled. Data for the first confirmed RSVH during the season (+1 month) were analyzed. Incidence and hospitalization rate per 100 patient-seasons, intensive care unit admission and length of stay (LOS), oxygen support, mechanical ventilation and overall hospital LOS were assessed.
Results: The pooled analysis comprised 7,820 infants; 267 experienced a confirmed RSVH at a median age of 8.4 weeks. The crude pooled RSVH incidence rate was 3.41% and the rate per 100 patient-seasons was 4.52. Median hospital LOS was 5.7 days. A total of 22.2% of infants required intensive care unit admission for a median LOS of 8.3 days. A total of 70.4% received supplemental oxygen support for a median of 4.9 days, and 12.7% required mechanical ventilation for a median of 4.8 days.
Conclusions: The burden of RSVH in moderate-late, 33-35 weeks' wGA preterm infants without comorbidities born during the viral season in Northern Hemisphere countries is substantial. Severe cases required prolonged and invasive supportive therapy.
Conflict of interest statement
Funding support for this pooled database analysis was provided by AbbVie. E.J.A., X.C.-E., M.B., M.L., M.S.-P. and B.P. have received research funding and/or compensation as advisor/lecturer from AbbVie. E.J.A. has received research funding from MedImmune. B.R.-G. and J.F., working for Strategen, have previously received payment from AbbVie for work on various projects. E.R., P.V. and F.C. are former employees of AbbVie and may hold AbbVie stock or stock options. G.N. is an employee of AbbVie and may hold AbbVie stock or stock options. The authors have no conflicts of interest to disclose.
Figures
References
-
- Horn SD, Smout RJ. Effect of prematurity on respiratory syncytial virus hospital resource use and outcomes. J Pediatr. 2003;143(5 suppl):S133–S141. - PubMed
-
- Figueras-Aloy J, Carbonell-Estrany X, Quero J IRIS Study Group. Case-control study of the risk factors linked to respiratory syncytial virus infection requiring hospitalization in premature infants born at a gestational age of 33-35 weeks in Spain. Pediatr Infect Dis J. 2004;23:815–820. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
