

Obstetric Facility Quality and Newborn Mortality in Malawi: A Cross-Sectional Study
- PMID: 27755547
- PMCID: PMC5068819
- DOI: 10.1371/journal.pmed.1002151
Obstetric Facility Quality and Newborn Mortality in Malawi: A Cross-Sectional Study
Abstract
Background: Ending preventable newborn deaths is a global health priority, but efforts to improve coverage of maternal and newborn care have not yielded expected gains in infant survival in many settings. One possible explanation is poor quality of clinical care. We assess facility quality and estimate the association of facility quality with neonatal mortality in Malawi.
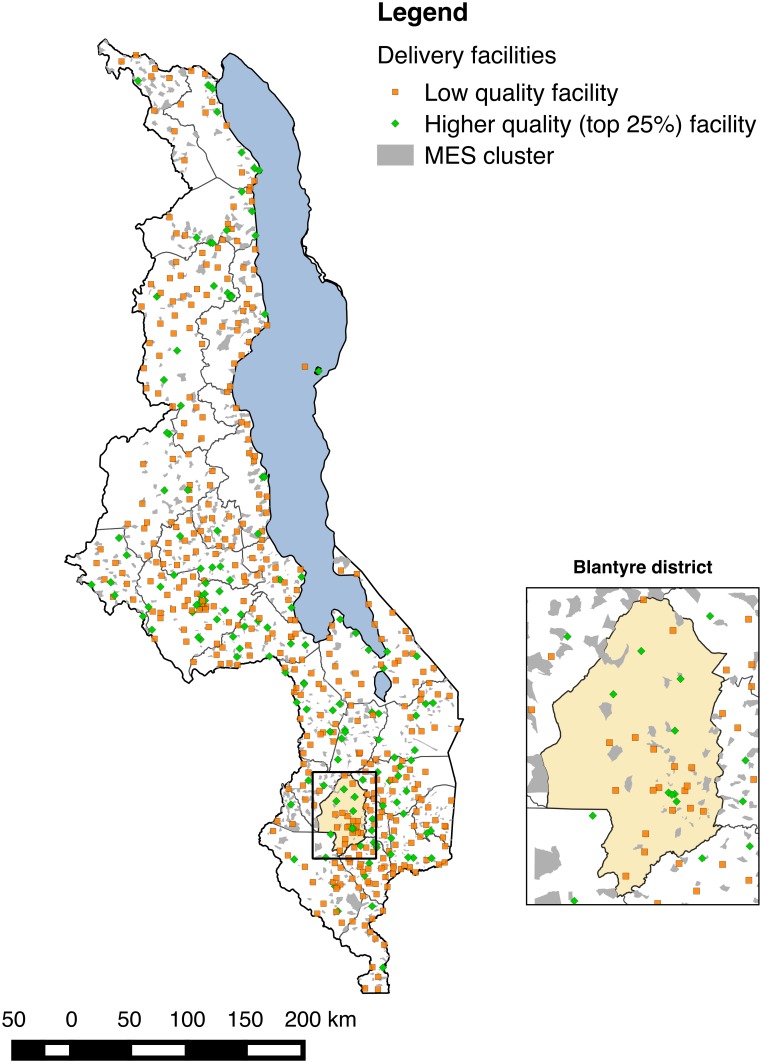
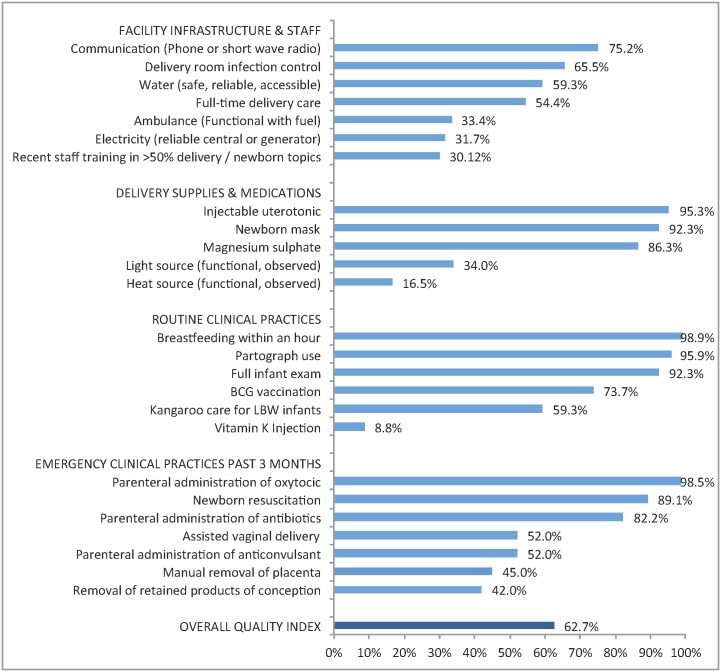
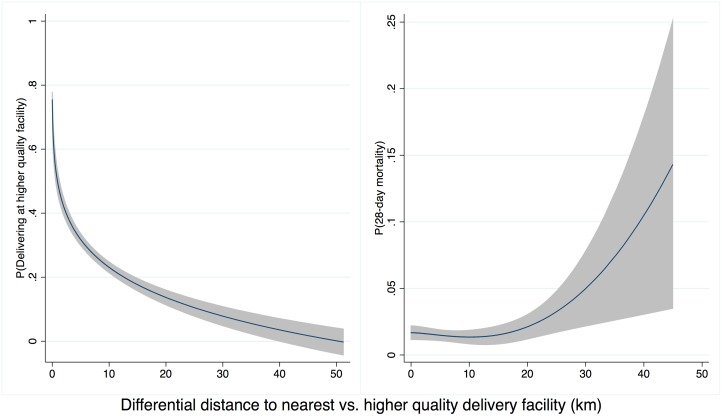
Methods and findings: Data on facility infrastructure as well as processes of routine and basic emergency obstetric care for all facilities in the country were obtained from 2013 Malawi Service Provision Assessment. Birth location and mortality for children born in the preceding two years were obtained from the 2013-2014 Millennium Development Goals Endline Survey. Facilities were classified as higher quality if they ranked in the top 25% of delivery facilities based on an index of 25 predefined quality indicators. To address risk selection (sicker mothers choosing or being referred to higher-quality facilities), we employed instrumental variable (IV) analysis to estimate the association of facility quality of care with neonatal mortality. We used the difference between distance to the nearest facility and distance to a higher-quality delivery facility as the instrument. Four hundred sixty-seven of the 540 delivery facilities in Malawi, including 134 rated as higher quality, were linked to births in the population survey. The difference between higher- and lower-quality facilities was most pronounced in indicators of basic emergency obstetric care procedures. Higher-quality facilities were located a median distance of 3.3 km further from women than the nearest delivery facility and were more likely to be in urban areas. Among the 6,686 neonates analyzed, the overall neonatal mortality rate was 17 per 1,000 live births. Delivery in a higher-quality facility (top 25%) was associated with a 2.3 percentage point lower newborn mortality (95% confidence interval [CI] -0.046, 0.000, p-value 0.047). These results imply a newborn mortality rate of 28 per 1,000 births at low-quality facilities and of 5 per 1,000 births at the top 25% of facilities, accounting for maternal and newborn characteristics. This estimate applies to newborns whose mothers would switch from a lower-quality to a higher-quality facility if one were more accessible. Although we did not find an indication of unmeasured associations between the instrument and outcome, this remains a potential limitation of IV analysis.
Conclusions: Poor quality of delivery facilities is associated with higher risk of newborn mortality in Malawi. A shift in focus from increasing utilization of delivery facilities to improving their quality is needed if global targets for further reductions in newborn mortality are to be achieved.
Conflict of interest statement
MEK is a member of the Editorial Board of PLOS Medicine.
Figures
Similar articles
-
The effects of changes in distance to nearest health facility on under-5 mortality and health care utilization in rural Malawi, 1980-1998.BMC Health Serv Res. 2020 Sep 24;20(1):899. doi: 10.1186/s12913-020-05738-w. BMC Health Serv Res. 2020. PMID: 32972395 Free PMC article.
-
Predicted effect of regionalised delivery care on neonatal mortality, utilisation, financial risk, and patient utility in Malawi: an agent-based modelling analysis.Lancet Glob Health. 2019 Jul;7(7):e932-e939. doi: 10.1016/S2214-109X(19)30170-6. Lancet Glob Health. 2019. PMID: 31200892 Free PMC article.
-
Distance to care, facility delivery and early neonatal mortality in Malawi and Zambia.PLoS One. 2012;7(12):e52110. doi: 10.1371/journal.pone.0052110. Epub 2012 Dec 27. PLoS One. 2012. PMID: 23300599 Free PMC article.
-
Place of delivery and perinatal mortality in Kenya.Semin Perinatol. 2019 Aug;43(5):252-259. doi: 10.1053/j.semperi.2019.03.014. Epub 2019 Mar 16. Semin Perinatol. 2019. PMID: 31104765 Review.
-
Scaling up quality care for mothers and newborns around the time of birth: an overview of methods and analyses of intervention-specific bottlenecks and solutions.BMC Pregnancy Childbirth. 2015;15 Suppl 2(Suppl 2):S1. doi: 10.1186/1471-2393-15-S2-S1. Epub 2015 Sep 11. BMC Pregnancy Childbirth. 2015. PMID: 26390820 Free PMC article. Review.
Cited by
-
Impact of newly constructed primary healthcare centres on antenatal care attendance, facility delivery and all-cause mortality: quasi-experimental evidence from Taabo health and demographic surveillance system, Côte d'Ivoire.BMJ Open. 2022 Jan 31;12(1):e054355. doi: 10.1136/bmjopen-2021-054355. BMJ Open. 2022. PMID: 35105634 Free PMC article.
-
The association between institutional delivery and neonatal mortality based on the quality of maternal and newborn health system in India.Sci Rep. 2022 Apr 13;12(1):6220. doi: 10.1038/s41598-022-10214-y. Sci Rep. 2022. PMID: 35418654 Free PMC article.
-
Resource availability and barriers to delivering quality care for newborns in hospitals in the southern region of Malawi: A multisite observational study.PLOS Glob Public Health. 2022 Dec 5;2(12):e0001333. doi: 10.1371/journal.pgph.0001333. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962885 Free PMC article.
-
Implementation of an international standardized set of outcome indicators in pregnancy and childbirth in Kenya: Utilizing mobile technology to collect patient-reported outcomes.PLoS One. 2019 Oct 16;14(10):e0222978. doi: 10.1371/journal.pone.0222978. eCollection 2019. PLoS One. 2019. PMID: 31618249 Free PMC article.
-
Hospital delivery and neonatal mortality in 37 countries in sub-Saharan Africa and South Asia: An ecological study.PLoS Med. 2021 Dec 1;18(12):e1003843. doi: 10.1371/journal.pmed.1003843. eCollection 2021 Dec. PLoS Med. 2021. PMID: 34851947 Free PMC article.
References
-
- United Nations Development Program. Sustainable Development Goals. Geneva, Switzerland: United Nations, 2015.
-
- Wang H, Liddell CA, Coates MM, Mooney MD, Levitz CE, Schumacher AE, et al. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet (London, England). 2014;384(9947):957–79. Epub 2014/05/07. 10.1016/s0140-6736(14)60497-9 - DOI - PMC - PubMed
-
- Child Mortality Estimates. In: UN Inter-agency Group for Child Mortality, editor.: UNICEF; 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
