

Sterilizing Activity of Fully Oral Intermittent Regimens against Mycobacterium Ulcerans Infection in Mice
- PMID: 27755552
- PMCID: PMC5068736
- DOI: 10.1371/journal.pntd.0005066
Sterilizing Activity of Fully Oral Intermittent Regimens against Mycobacterium Ulcerans Infection in Mice
Abstract
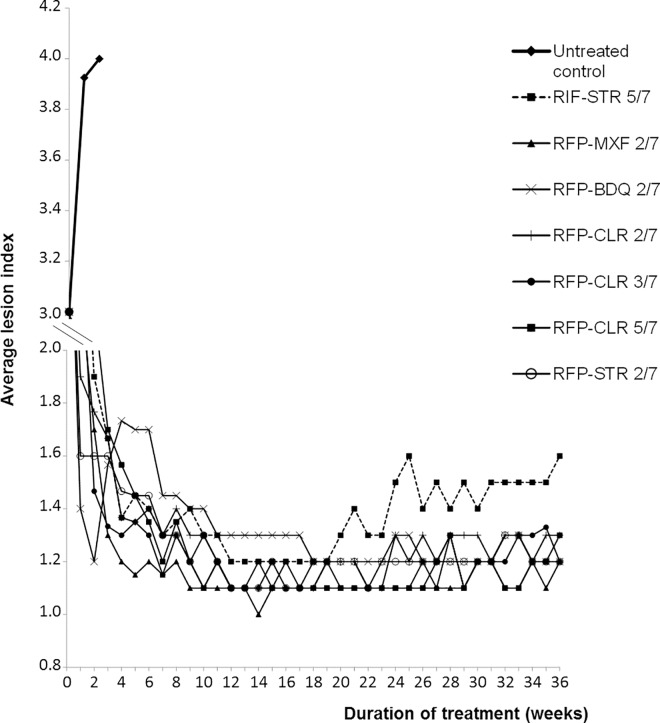
Background: The treatment of Buruli ulcer (BU) that is caused by Mycobacterium ulcerans, is currently based on a daily administration of rifampin and streptomycin (RIF-STR). A fully oral intermittent regimen would greatly simplify its treatment on the field.
Methodology/principal findings: The objective of this study was to assess the bactericidal and sterilizing activities of intermittent oral regimens in a murine model of established M. ulcerans infection. Regimens combining rifapentine (RFP 20 mg/kg) with either moxifloxacin (MXF 200 mg/kg), clarithromycin (CLR 100 mg/kg) or bedaquiline (BDQ 25 mg/kg) were administrated twice (2/7) or three (only for RFP-CLR 3/7) times weekly during 8 weeks. The bactericidal but also the sterilizing activities of these four intermittent oral regimens were at least as good as those obtained with control weekdays regimens, i.e. RFP-CLR 5/7 or RIF-STR 5/7. A single mouse from the RFP-MFX 2/7 group had culture-positive relapse at the end of the 28 weeks following treatment completion among the 157 mice treated with one of the four intermittent regimens (40 RFP-CLR 2/7, 39 RFP-CLR 3/7, 39 RFP-MXF 2/7, 39 RFP-BDQ 2/7).
Conclusions/significance: These results open the door for a fully intermittent oral drug regimen for BU treatment avoiding intramuscular injections and facilitating supervision by health care workers.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Activities of rifampin, Rifapentine and clarithromycin alone and in combination against mycobacterium ulcerans disease in mice.PLoS Negl Trop Dis. 2011 Jan 4;5(1):e933. doi: 10.1371/journal.pntd.0000933. PLoS Negl Trop Dis. 2011. PMID: 21245920 Free PMC article.
-
Shortening Buruli Ulcer Treatment with Combination Therapy Targeting the Respiratory Chain and Exploiting Mycobacterium ulcerans Gene Decay.Antimicrob Agents Chemother. 2019 Jun 24;63(7):e00426-19. doi: 10.1128/AAC.00426-19. Print 2019 Jul. Antimicrob Agents Chemother. 2019. PMID: 31036687 Free PMC article.
-
High-Dose Rifamycins Enable Shorter Oral Treatment in a Murine Model of Mycobacterium ulcerans Disease.Antimicrob Agents Chemother. 2019 Jan 29;63(2):e01478-18. doi: 10.1128/AAC.01478-18. Print 2019 Feb. Antimicrob Agents Chemother. 2019. PMID: 30455239 Free PMC article.
-
Pharmacologic management of Mycobacterium ulcerans infection.Expert Rev Clin Pharmacol. 2020 Apr;13(4):391-401. doi: 10.1080/17512433.2020.1752663. Epub 2020 Apr 20. Expert Rev Clin Pharmacol. 2020. PMID: 32310683 Free PMC article. Review.
-
Buruli Ulcer: Review of a Neglected Skin Mycobacterial Disease.J Clin Microbiol. 2018 Mar 26;56(4):e01507-17. doi: 10.1128/JCM.01507-17. Print 2018 Apr. J Clin Microbiol. 2018. PMID: 29343539 Free PMC article. Review.
Cited by
-
Triple oral beta-lactam containing therapy for Buruli ulcer treatment shortening.PLoS Negl Trop Dis. 2019 Jan 28;13(1):e0007126. doi: 10.1371/journal.pntd.0007126. eCollection 2019 Jan. PLoS Negl Trop Dis. 2019. PMID: 30689630 Free PMC article.
-
Toward a Single-Dose Cure for Buruli Ulcer.Antimicrob Agents Chemother. 2020 Aug 20;64(9):e00727-20. doi: 10.1128/AAC.00727-20. Print 2020 Aug 20. Antimicrob Agents Chemother. 2020. PMID: 32631818 Free PMC article.
-
Skin and Soft Tissue Infections Due to Nontuberculous Mycobacteria.Curr Infect Dis Rep. 2018 Mar 19;20(4):6. doi: 10.1007/s11908-018-0611-3. Curr Infect Dis Rep. 2018. PMID: 29556857 Review.
-
Telacebec (Q203)-containing intermittent oral regimens sterilized mice infected with Mycobacterium ulcerans after only 16 doses.PLoS Negl Trop Dis. 2020 Aug 31;14(8):e0007857. doi: 10.1371/journal.pntd.0007857. eCollection 2020 Aug. PLoS Negl Trop Dis. 2020. PMID: 32866170 Free PMC article.
-
Treatment for Buruli ulcer: the long and winding road to antimicrobials-first.Cochrane Database Syst Rev. 2018 Dec 17;12(12):ED000128. doi: 10.1002/14651858.ED000128. Cochrane Database Syst Rev. 2018. PMID: 30556580 Free PMC article. No abstract available.
References
-
- World Health Organization. Buruli ulcer: progress report, 2004–2008. Wkly Epidemiol Rec. 2008;83: 145–156. - PubMed
-
- Kibadi K, Mputu-Yamba JB, Mokassa B, Panda M, Muyembe-Tamfum JJ. [Relapse after surgical treatment of mycobacterium ulcerans infection (buruli ulcer): study of risk factors in 84 patients in the Democratic Republic of the Congo]. Médecine Trop Rev Corps Santé Colon. 2009;69: 471–474. - PubMed
-
- WHO | Provisional guidance on the role of specific antibiotics in the management of Mycobacterium ulcerans disease (Buruli ulcer). In: WHO [Internet]. [cited 17 Apr 2014]. Available: http://www.who.int/buruli/information/antibiotics/en/
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
