

Assessing Program Coverage of Two Approaches to Distributing a Complementary Feeding Supplement to Infants and Young Children in Ghana
- PMID: 27755554
- PMCID: PMC5068796
- DOI: 10.1371/journal.pone.0162462
Assessing Program Coverage of Two Approaches to Distributing a Complementary Feeding Supplement to Infants and Young Children in Ghana
Abstract
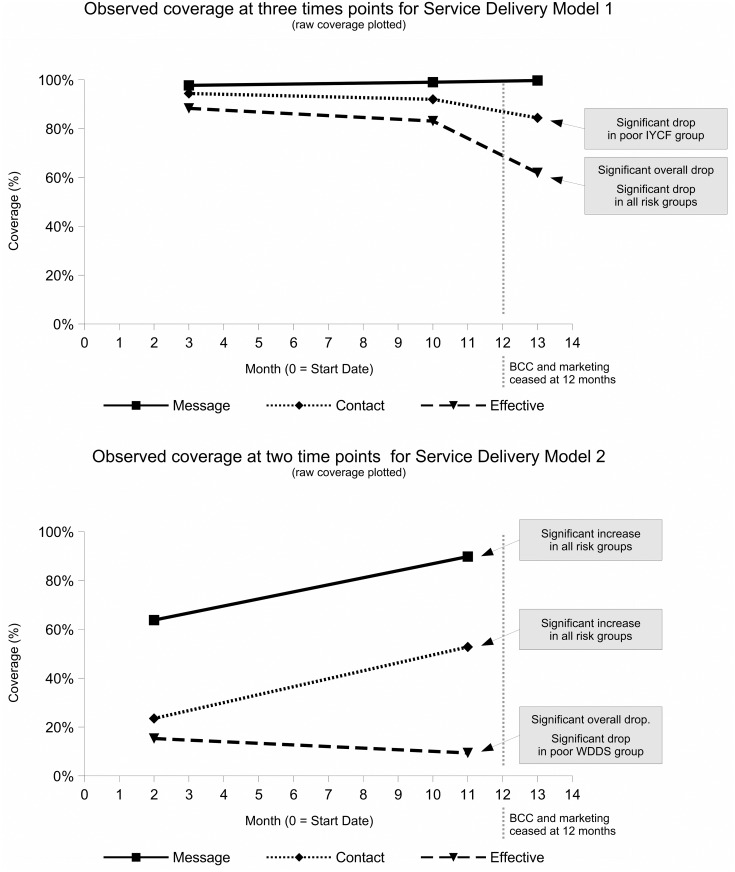
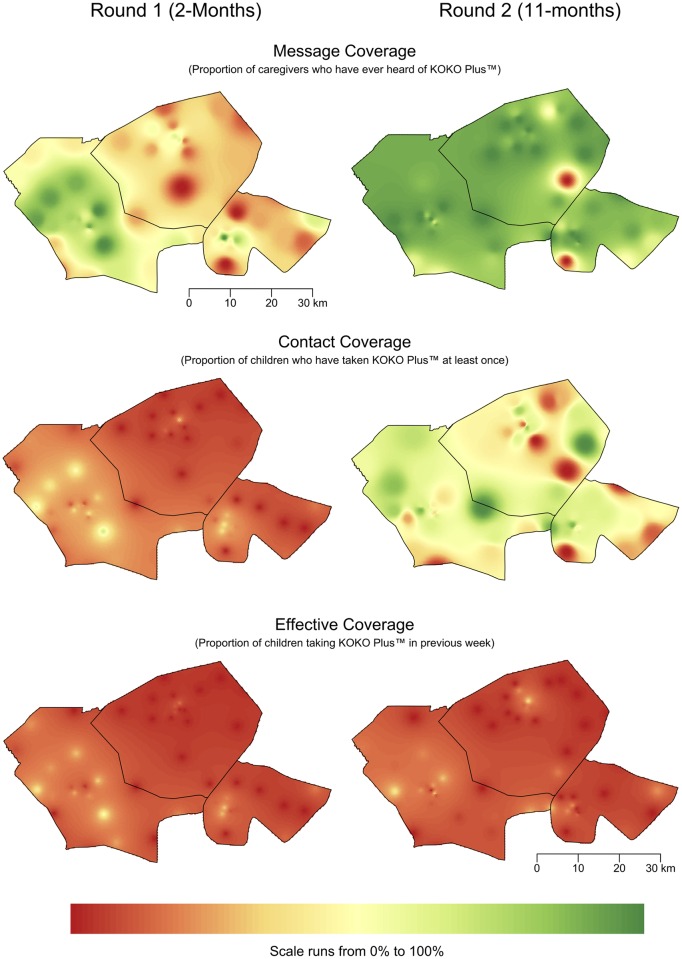
The work reported here assesses the coverage achieved by two sales-based approaches to distributing a complementary food supplement (KOKO Plus™) to infants and young children in Ghana. Delivery Model 1 was conducted in the Northern Region of Ghana and used a mixture of health extension workers (delivering behavior change communications and demand creation activities at primary healthcare centers and in the community) and petty traders recruited from among beneficiaries of a local microfinance initiative (responsible for the sale of the complementary food supplement at market stalls and house to house). Delivery Model 2 was conducted in the Eastern Region of Ghana and used a market-based approach, with the product being sold through micro-retail routes (i.e., small shops and roadside stalls) in three districts supported by behavior change communications and demand creation activities led by a local social marketing company. Both delivery models were implemented sub-nationally as 1-year pilot programs, with the aim of informing the design of a scaled-up program. A series of cross-sectional coverage surveys was implemented in each program area. Results from these surveys show that Delivery Model 1 was successful in achieving and sustaining high (i.e., 86%) effective coverage (i.e., the child had been given the product at least once in the previous 7 days) during implementation. Effective coverage fell to 62% within 3 months of the behavior change communications and demand creation activities stopping. Delivery Model 2 was successful in raising awareness of the product (i.e., 90% message coverage), but effective coverage was low (i.e., 9.4%). Future programming efforts should use the health extension / microfinance / petty trader approach in rural settings and consider adapting this approach for use in urban and peri-urban settings. Ongoing behavior change communications and demand creation activities is likely to be essential to the continued success of such programming.
Conflict of interest statement
All co-authors have full freedom regarding the publication of results from this study. There are no financial conflicts of interest to declare. GJA is employed by the Global Alliance to Improve Nutrition (GAIN); NS and SG are employed by the International Nutrition Foundation; EG, KS, and AN are employed by Valid International Ltd (a public health consultancy firm); NAB, KT-D, and DS are employed by the University of Ghana; MN and AA are employed by CARE International in Ghana; RB is employed by Exp Social Marketing; EF is employed by the Ghana Health Service; YT and SK are employed by Ajinomoto Co., Inc, Tokyo, Japan; MM is director of Brixton Health (a public health consultancy firm). These affiliations do not alter the authors' adherence to all the PLoS ONE policies on sharing data and materials.
Figures
Similar articles
-
Improving complementary feeding in Ghana: reaching the vulnerable through innovative business--the case of KOKO Plus.Ann N Y Acad Sci. 2014 Dec;1331:76-89. doi: 10.1111/nyas.12596. Ann N Y Acad Sci. 2014. PMID: 25514865
-
Coverage of Nutrition Interventions Intended for Infants and Young Children Varies Greatly across Programs: Results from Coverage Surveys in 5 Countries.J Nutr. 2017 May;147(5):995S-1003S. doi: 10.3945/jn.116.245407. Epub 2017 Apr 12. J Nutr. 2017. PMID: 28404839 Free PMC article. Review.
-
High Awareness but Low Coverage of a Locally Produced Fortified Complementary Food in Abidjan, Côte d'Ivoire: Findings from a Cross-Sectional Survey.PLoS One. 2016 Nov 8;11(11):e0166295. doi: 10.1371/journal.pone.0166295. eCollection 2016. PLoS One. 2016. PMID: 27824917 Free PMC article.
-
Development and Sensory Shelf-Life Testing of KOKO Plus: A Food Supplement for Improving the Nutritional Profiles of Traditional Complementary Foods.Food Nutr Bull. 2019 Sep;40(3):340-356. doi: 10.1177/0379572119848290. Epub 2019 Jun 26. Food Nutr Bull. 2019. PMID: 31242762
-
Marketing complementary foods and supplements in Burkina Faso, Madagascar, and Vietnam: lessons learned from the Nutridev program.Food Nutr Bull. 2010 Jun;31(2 Suppl):S154-67. doi: 10.1177/15648265100312S208. Food Nutr Bull. 2010. PMID: 20715600 Review.
Cited by
-
Changes of Plasma Amino Acid Profiles in Infants With a Nutrient-Fortified Complementary Food Supplement: Evidence From a 12-Month Single-Blind Cluster-Randomized Controlled Trial.Front Nutr. 2021 Sep 30;8:606002. doi: 10.3389/fnut.2021.606002. eCollection 2021. Front Nutr. 2021. PMID: 34660654 Free PMC article.
-
Multisectoral interventions for urban health in Africa: a mixed-methods systematic review.Glob Health Action. 2024 Dec 31;17(1):2325726. doi: 10.1080/16549716.2024.2325726. Epub 2024 Apr 5. Glob Health Action. 2024. PMID: 38577879 Free PMC article.
-
Variance estimation for effective coverage measures: A simulation study.J Glob Health. 2020 Jun;10(1):010506. doi: 10.7189/jogh.10.010506. J Glob Health. 2020. PMID: 32257160 Free PMC article.
-
Mixed methods evaluation explains bypassing of vouchers in micronutrient powder trial in Mozambique.Matern Child Nutr. 2019 Oct;15(S5):e12718. doi: 10.1111/mcn.12718. Matern Child Nutr. 2019. PMID: 31622037 Free PMC article.
-
Experiences and lessons learned for delivery of micronutrient powders interventions.Matern Child Nutr. 2017 Sep;13 Suppl 1(Suppl 1):e12495. doi: 10.1111/mcn.12495. Matern Child Nutr. 2017. PMID: 28960878 Free PMC article.
References
-
- WHO/UNICEF. 2003. Global strategy on infant and young child feeding. Geneva, World Health Organization. (http://www.who.int/maternal_child_adolescent/documents/9241562218/en/, accessed on: March 6, 2015).
-
- Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: a pooled analysis. WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality. Lancet. 2000;355(9202):451–5. . - PubMed
-
- Daelmans B, Mangasaryan N, Martines J, Saadeh R, Casanovas C, Arabi M. Strengthening actions to improve feeding of infants and young children 6 to 23 months of age: summary of a recent World Health Organization/UNICEF technical meeting, Geneva, 6–9 October 2008. Food and nutrition bulletin. 2009;30(2 Suppl):S236–8. . - PubMed
-
- Ghana Statistical Service, 2011. Ghana Multiple Indicator Cluster Survey with an Enhanced Malaria Module and Biomarker, 2011, Final Report. Accra, Ghana. https://goo.gl/UJzQVg. Accessed 20 June 2015.
-
- Ghana Statistical Service, Ghana Health Service, and ICF Macro. Ghana Demographic and Health Survey 2008 [Dataset]. Data Extract from GHIR5A and GHHR5A.SAV. Integrated Demographic and Health Series (IDHS), version 1.0, Minnesota Population Center and ICF International [Distributors]. Accessed from http://idhsdata.org
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
