

Untargeted Metabolomic Analysis of Amniotic Fluid in the Prediction of Preterm Delivery and Bronchopulmonary Dysplasia
- PMID: 27755564
- PMCID: PMC5068788
- DOI: 10.1371/journal.pone.0164211
Untargeted Metabolomic Analysis of Amniotic Fluid in the Prediction of Preterm Delivery and Bronchopulmonary Dysplasia
Abstract
Objective: Bronchopulmonary dysplasia (BPD) is a serious complication associated with preterm birth. A growing body of evidence suggests a role for prenatal factors in its pathogenesis. Metabolomics allows simultaneous characterization of low molecular weight compounds and may provide a picture of such a complex condition. The aim of this study was to evaluate whether an unbiased metabolomic analysis of amniotic fluid (AF) can be used to investigate the risk of spontaneous preterm delivery (PTD) and BPD development in the offspring.
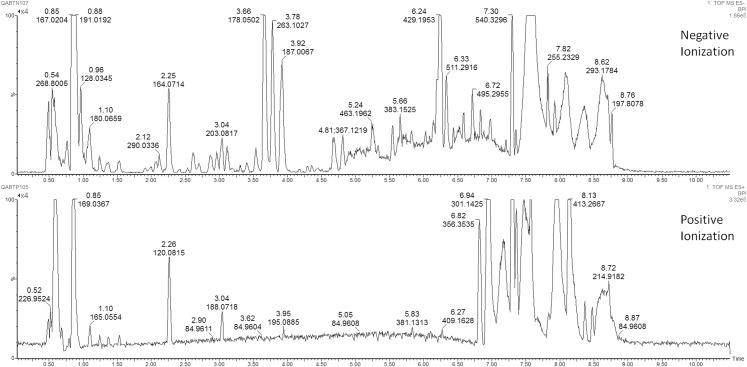
Study design: We conducted an exploratory study on 32 infants born from mothers who had undergone an amniocentesis between 21 and 28 gestational weeks because of spontaneous preterm labor with intact membranes. The AF samples underwent untargeted metabolomic analysis using mass spectrometry combined with ultra-performance liquid chromatography. The data obtained were analyzed using multivariate and univariate statistical data analysis tools.
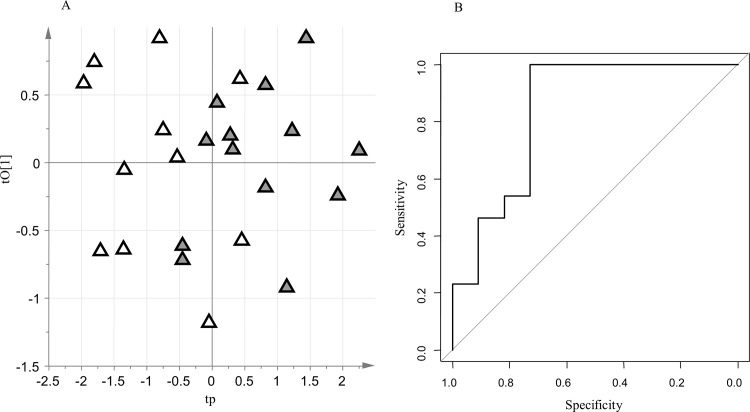
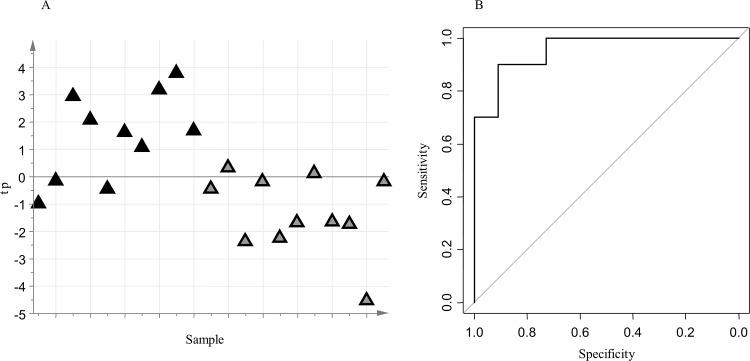
Results: Orthogonally Constrained Projection to Latent Structures-Discriminant Analysis (oCPLS2-DA) excluded effects on data modelling of crucial clinical variables. oCPLS2-DA was able to find unique differences in select metabolites between term (n = 11) and preterm (n = 13) deliveries (negative ionization data set: R2 = 0.47, mean AUC ROC in prediction = 0.65; positive ionization data set: R2 = 0.47, mean AUC ROC in prediction = 0.70), and between PTD followed by the development of BPD (n = 10), and PTD without BPD (n = 11) (negative data set: R2 = 0.48, mean AUC ROC in prediction = 0.73; positive data set: R2 = 0.55, mean AUC ROC in prediction = 0.71).
Conclusions: This study suggests that amniotic fluid metabolic profiling may be promising for identifying spontaneous preterm birth and fetuses at risk for developing BPD. These findings support the hypothesis that some prenatal metabolic dysregulations may play a key role in the pathogenesis of PTD and the development of BPD.
Conflict of interest statement
The authors have no conflicts of interest and no financial relationships relevant to this article to disclose. S-IN Soluzioni Informatiche did not provide employment, consultancy, patents, products in development, or marketed products related to this article, as well as financial support in the form of authors' salaries or research materials. This commercial affiliation (MS) does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
