

Single-incision versus standard multi-incision laparoscopic colectomy in patients with malignant or benign colonic disease: a systematic review, meta-analysis and assessment of the evidence
- PMID: 27756272
- PMCID: PMC5070079
- DOI: 10.1186/s12893-016-0187-5
Single-incision versus standard multi-incision laparoscopic colectomy in patients with malignant or benign colonic disease: a systematic review, meta-analysis and assessment of the evidence
Abstract
Background: Single-incision laparoscopic colectomy (SILC) requires only one umbilical port site and (depending on technique) a specimen extraction site. The aim of this study was the assessment of the available evidence for the comparison of SILC to conventional multi-port laparoscopic colectomy (MLC) in adult patients, in whom elective colectomy is indicated because of malignant or benign disease. First, previous meta-analyses on this topic were assessed. Secondly, a systematic review and meta-analysis of randomised controlled trials, was performed.
Methods: Electronic literature searches (CENTRAL, MEDLINE and EMBASE; up to March 2016) were performed. Additionally, we searched clinical trials registries and abstracts from surgical society meetings. For meta-analysis, risk ratios (RR) or mean differences (MD) with 95 % confidence intervals were calculated and pooled. The quality of previous meta-analyses was evaluated against established criteria (AMSTAR) and their reported results were investigated for consistency.
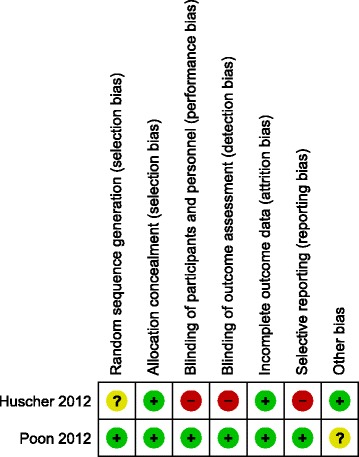
Results: We identified 6 previous meta-analyses of mostly low methodological quality (AMSTAR total score: 2 - 5 out of 11 items). To fill the evidence gaps, all these meta-analyses had included non-randomised studies, but usually without assessing their risk of bias. In our systematic review and meta-analysis of randomised controlled trials exclusively, we included two randomised controlled trials with a total of 82 colorectal cancer patients. There was insufficient evidence to clarify whether SILC leads to less local complications (RR = 0.52, 95 % CI 0.14 - 1.94) or lower mortality (1 death per treatment group). Length of hospital stay was significantly shorter in the SILC group (MD = -1.20 days, 95 % CI -1.95 to -0.44). One of the two studies found postoperative pain intensity to be lower at the first day. We also identified 7 ongoing trials with a total sample size of over 1000 patients.
Conclusion: The currently available study results are too sparse to detect (or rule out) relevant differences between SILC and MLC. The quality of the current evidence is low, and the additional analysis of non-randomised data attempts, but does not solve this problem. SILC should still be considered as an experimental procedure, since the evidence of well-designed randomised controlled trials is too sparse to allow any recommendation.
Keywords: Colon; Laparoscopy; Mini-invasive; Single port; Surgery.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
