

Trials based on specific fracture configuration and surgical procedures likely to be more relevant for decision making in the management of fractures of the proximal humerus: Findings of a meta-analysis
- PMID: 27756738
- PMCID: PMC5086838
- DOI: 10.1302/2046-3758.510.2000638
Trials based on specific fracture configuration and surgical procedures likely to be more relevant for decision making in the management of fractures of the proximal humerus: Findings of a meta-analysis
Abstract
Objectives: The objective of this study was to perform a meta-analysis of all randomised controlled trials (RCTs) comparing surgical and non-surgical management of fractures of the proximal humerus, and to determine whether further analyses based on complexity of fracture, or the type of surgical intervention, produced disparate findings on patient outcomes.
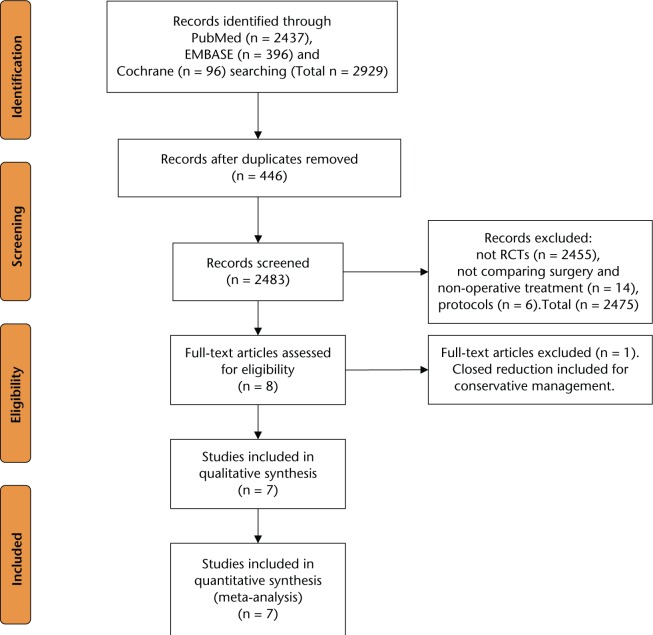
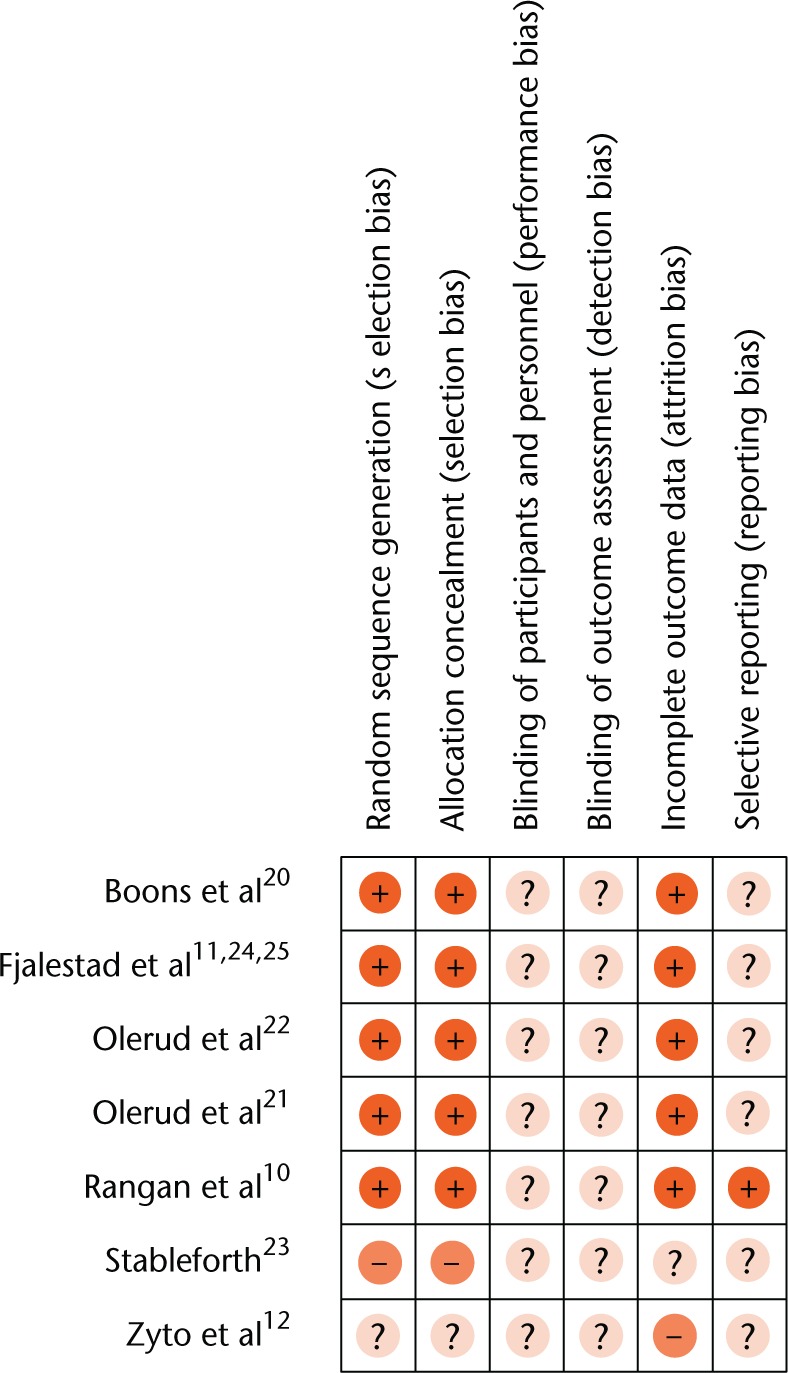
Methods: A systematic review of the literature was performed identifying all RCTs that compared surgical and non-surgical management of fractures of the proximal humerus. Meta-analysis of clinical outcomes was performed where possible. Subgroup analysis based on the type of fracture, and a sensitivity analysis based on the type of surgical intervention, were also performed.
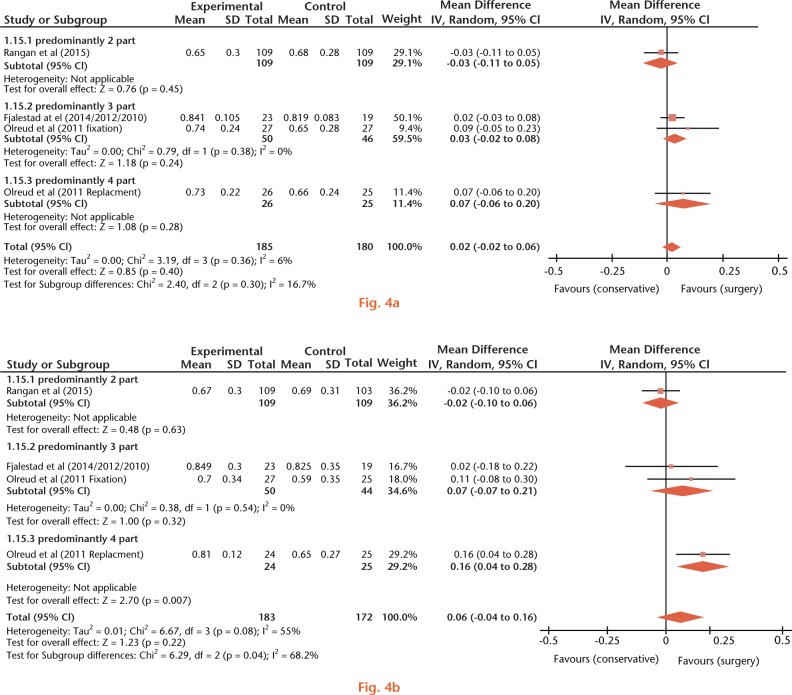
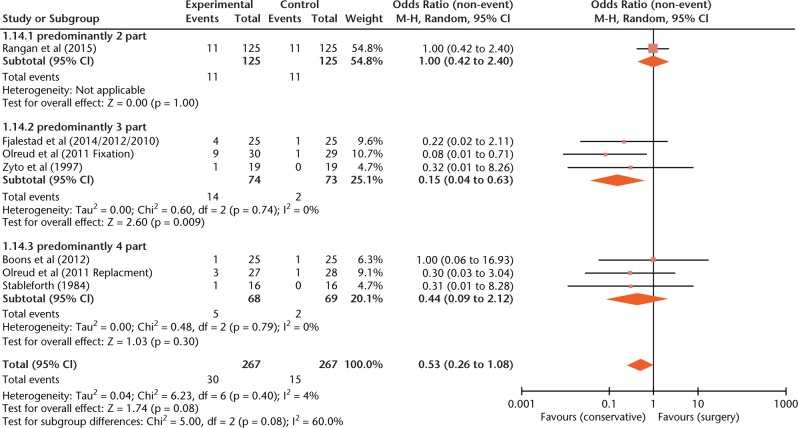
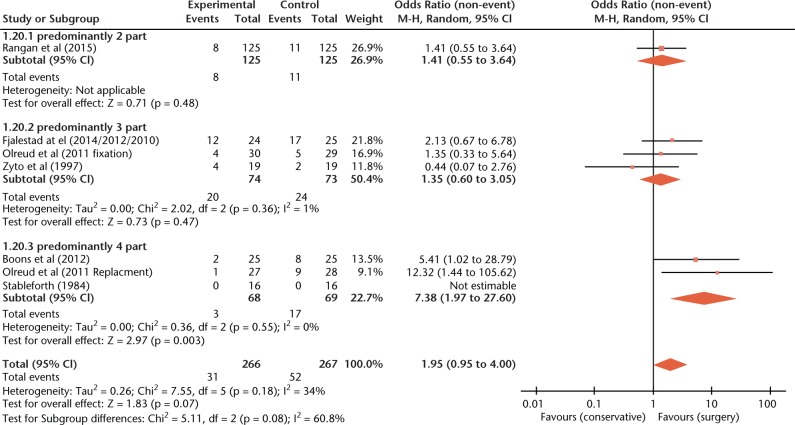
Results: Seven studies including 528 patients were included. The overall meta-analysis found that there was no difference in clinical outcomes. However, subgroup and sensitivity analyses found improved patient outcomes for more complex fractures managed surgically. Four-part fractures that underwent surgery had improved long-term health utility scores (mean difference, MD 95% CI 0.04 to 0.28; p = 0.007). They were also less likely to result in osteoarthritis, osteonecrosis and non/malunion (OR 7.38, 95% CI 1.97 to 27.60; p = 0.003). Another significant subgroup finding was that secondary surgery was more common for patients that underwent internal fixation compared with conservative management within the studies with predominantly three-part fractures (OR 0.15, 95% CI 0.04 to 0.63; p = 0.009).
Conclusion: This meta-analysis has demonstrated that differences in the type of fracture and surgical treatment result in outcomes that are distinct from those generated from analysis of all types of fracture and surgical treatments grouped together. This has important implications for clinical decision making and should highlight the need for future trials to adopt more specific inclusion criteria.Cite this article: S. Sabharwal, N. K. Patel, D. Griffiths, T. Athanasiou, C. M. Gupte, P. Reilly. Trials based on specific fracture configuration and surgical procedures likely to be more relevant for decision making in the management of fractures of the proximal humerus: Findings of a meta-analysisBone Joint Res 2016;5:470-480. DOI: 10.1302/2046-3758.510.2000638.
Keywords: Meta-analysis; Proximal humerus fracture.
© 2016 Sabharwal et al.
Conflict of interest statement
ICMJE conflict of interest: None declared
Figures
References
-
- Baron JA, Karagas M, Barrett J, et al. Basic epidemiology of fractures of the upper and lower limb among Americans over 65 years of age. Epidemiology 1996;7:612-618. - PubMed
-
- Kannus P, Palvanen M, Niemi S, et al. Osteoporotic fractures of the proximal humerus in elderly Finnish persons: sharp increase in 1970-1998 and alarming projections for the new millennium. Acta Orthop Scand 2000;71:465-470. - PubMed
-
- Kim SH, Szabo RM, Marder RA. Epidemiology of humerus fractures in the United States: nationwide emergency department sample, 2008. Arthritis Care Res (Hoboken) 2012;64:407-414. - PubMed
-
- Court-Brown CM, Garg A, McQueen MM. The epidemiology of proximal humeral fractures. Acta Orthop Scand 2001;72:365-371. - PubMed
-
- Majed A, Macleod I, Bull AM, et al. Proximal humeral fracture classification systems revisited. J Shoulder Elbow Surg 2011;20:1125-1132. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
