

Identifying Important Gaps in Randomized Controlled Trials of Adult Cardiac Arrest Treatments: A Systematic Review of the Published Literature
- PMID: 27756794
- PMCID: PMC5339040
- DOI: 10.1161/CIRCOUTCOMES.116.002916
Identifying Important Gaps in Randomized Controlled Trials of Adult Cardiac Arrest Treatments: A Systematic Review of the Published Literature
Abstract
Background: Cardiac arrest is a major public health concern worldwide. The extent and types of randomized controlled trials (RCT)-our most reliable source of clinical evidence-conducted in these high-risk patients over recent years are largely unknown.
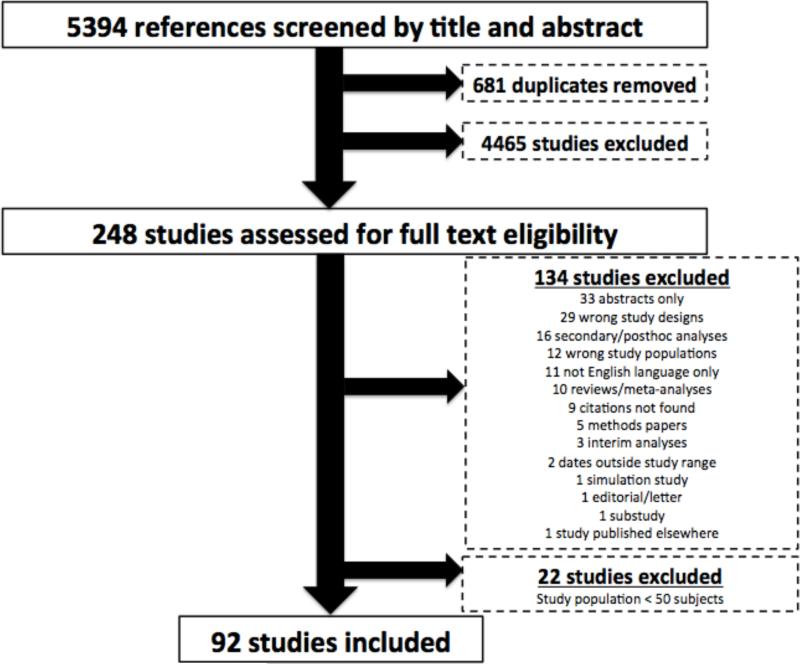
Methods and results: We performed a systematic review, identifying all RCTs published in PubMed, EMBASE, Scopus, Web of Science, and the Cochrane Library from 1995 to 2014 that focused on the acute treatment of nontraumatic cardiac arrest in adults. We then extracted data on the setting of study populations, types and timing of interventions studied, risk of bias, outcomes reported, and how these factors have changed over time. Over this 20-year period, 92 RCTs were published containing 64 309 patients (median, 225.5 per trial). Of these, 81 RCTs (88.0%) involved out-of-hospital cardiac arrest, whereas 4 (4.3%) involved in-hospital cardiac arrest and 7 (7.6%) included both. Eighteen RCTs (19.6%) were performed in the United States, 68 (73.9%) were performed outside the United States, and 6 (6.5%) were performed in both settings. Thirty-eight RCTs (41.3%) evaluated drug therapy, 39 (42.4%) evaluated device therapy, and 15 (16.3%) evaluated protocol improvements. Seventy-four RCTs (80.4%) examined interventions during the cardiac arrest, 15 (16.3%) examined post cardiac arrest treatment, and 3 (3.3%) studied both. Overall, reporting of the risk of bias was limited. The most common outcome reported was return of spontaneous circulation: 86 (93.5%) with only 22 (23.9%) reporting survival beyond 6 months. Fifty-three RCTs (57.6%) reported global ordinal outcomes, whereas 15 (16.3%) reported quality-of-life. RCTs in the past 5 years were more likely to be focused on protocol improvements and postcardiac arrest care.
Conclusions: Important gaps in RCTs of cardiac arrest treatments exist, especially those examining in-hospital cardiac arrest, protocol improvement, postcardiac arrest care, and long-term or quality-of-life outcomes.
Keywords: cardiopulmonary resuscitation; health services research; heart arrest; randomized controlled trial; resuscitation.
© 2016 American Heart Association, Inc.
Figures
References
-
- Writing Group M. Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jimenez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB. American Heart Association Statistics C and Stroke Statistics S. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133:e38–60. - PubMed
-
- Graham R, McCoy MA, Schultz AM, editors. Strategies to Improve Cardiac Arrest Survival: A Time to Act. National Academies Press; Washington (DC): 2015. - PubMed
-
- Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation. 2010;81:1479–87. - PubMed
-
- Daya MR, Schmicker RH, Zive DM, Rea TD, Nichol G, Buick JE, Brooks S, Christenson J, MacPhee R, Craig A, Rittenberger JC, Davis DP, May S, Wigginton J, Wang H, Resuscitation Outcomes Consortium I Out-of-hospital cardiac arrest survival improving over time: Results from the Resuscitation Outcomes Consortium (ROC). Resuscitation. 2015;91:108–15. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
