

Endovascular therapy for acute ischaemic stroke: the Pragmatic Ischaemic Stroke Thrombectomy Evaluation (PISTE) randomised, controlled trial
- PMID: 27756804
- PMCID: PMC5256149
- DOI: 10.1136/jnnp-2016-314117
Endovascular therapy for acute ischaemic stroke: the Pragmatic Ischaemic Stroke Thrombectomy Evaluation (PISTE) randomised, controlled trial
Abstract
Objective: The Pragmatic Ischaemic Thrombectomy Evaluation (PISTE) trial was a multicentre, randomised, controlled clinical trial comparing intravenous thrombolysis (IVT) alone with IVT and adjunctive intra-arterial mechanical thrombectomy (MT) in patients who had acute ischaemic stroke with large artery occlusive anterior circulation stroke confirmed on CT angiography (CTA).
Design: Eligible patients had IVT started within 4.5 hours of stroke symptom onset. Those randomised to additional MT underwent thrombectomy using any Conformité Européene (CE)-marked device, with target interval times for IVT start to arterial puncture of <90 min. The primary outcome was the proportion of patients achieving independence defined by a modified Rankin Scale (mRS) score of 0-2 at day 90.
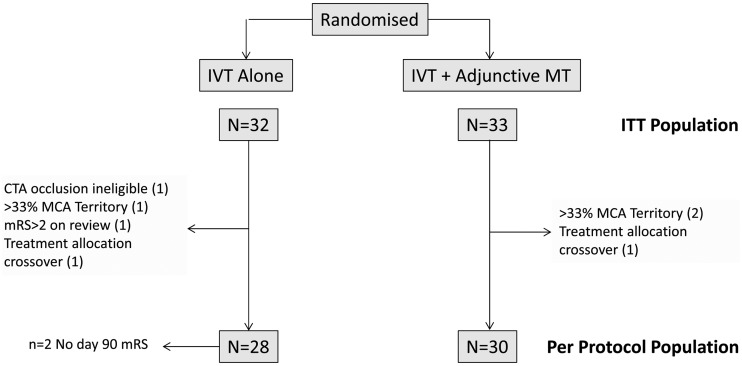
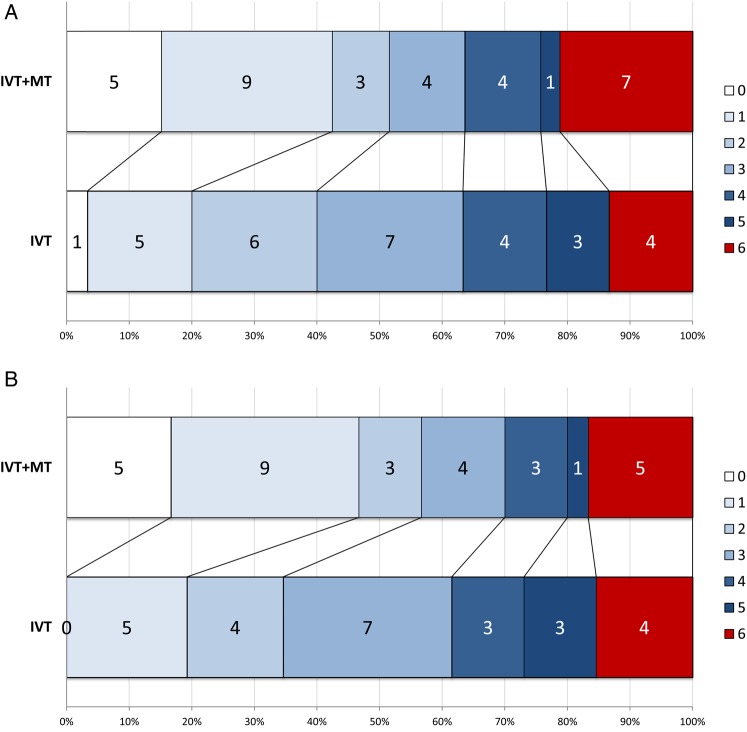
Results: Ten UK centres enrolled 65 patients between April 2013 and April 2015. Median National Institutes of Health Stroke Scale score was 16 (IQR 13-21). Median stroke onset to IVT start was 120 min. In the intention-to-treat analysis, there was no significant difference in disability-free survival at day 90 with MT (absolute difference 11%, adjusted OR 2.12, 95% CI 0.65 to 6.94, p=0.20). Secondary analyses showed significantly greater likelihood of full neurological recovery (mRS 0-1) at day 90 (OR 7.6, 95% CI 1.6 to 37.2, p=0.010). In the per-protocol population (n=58), the primary and most secondary clinical outcomes significantly favoured MT (absolute difference in mRS 0-2 of 22% and adjusted OR 4.9, 95% CI 1.2 to 19.7, p=0.021).
Conclusions: The trial did not find a significant difference between treatment groups for the primary end point. However, the effect size was consistent with published data and across primary and secondary end points. Proceeding as fast as possible to MT after CTA confirmation of large artery occlusion on a background of intravenous alteplase is safe, improves excellent clinical outcomes and, in the per-protocol population, improves disability-free survival.
Trial registration number: NCT01745692; Results.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
The Trial Steering Committee was chaired by GAF (Stroke Association funded phase) and by H Markus (HTA phase). JF was the lay representative on the Trial Steering Committee and participated in all trial design and management decisions. The Data Monitoring Committee was chaired by K R Lees (Stroke Association phase) and by T Robinson (HTA phase); and included S Lewis (Stroke Association phase), J Norrie (HTA phase) and A Molyneux (throughout).
Figures
References
-
- Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384:1929–35. 10.1016/S0140-6736(14)60584-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous