

Pain management in patients with Parkinson's disease: challenges and solutions
- PMID: 27757037
- PMCID: PMC5053370
- DOI: 10.2147/JMDH.S105857
Pain management in patients with Parkinson's disease: challenges and solutions
Abstract
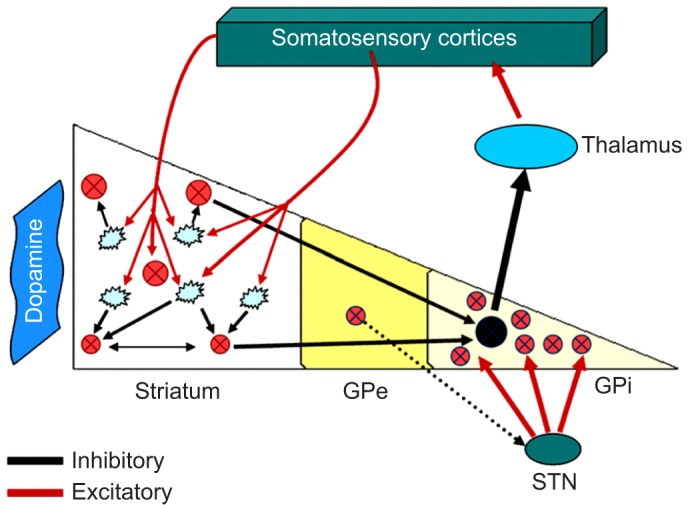
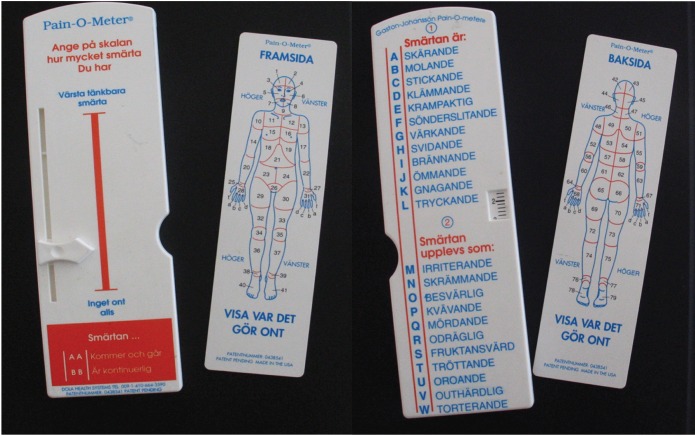
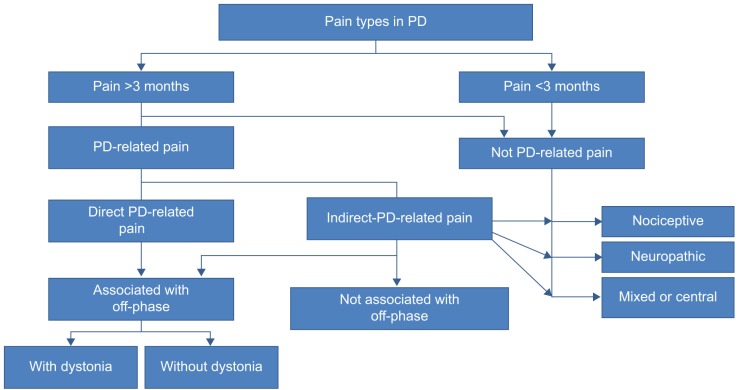
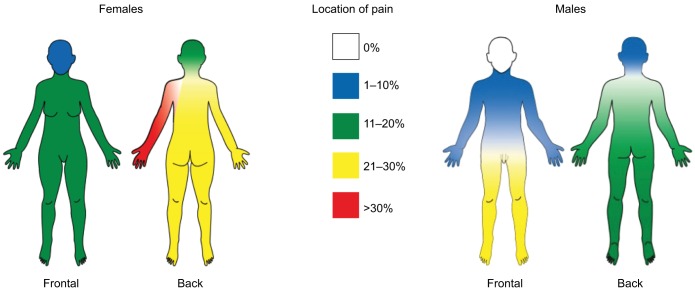
This review focuses on the diagnosis and management of Parkinson-related pain which is one of the more frequently reported nonmotor symptoms in Parkinson's disease (PD), which is the second most common neurodegenerative disease after Alzheimer's disease. Pain is ranked high by patients as a troublesome symptom in all stages of the disease. In early-stage PD, pain is rated as the most bothersome symptom. Knowledge of the correct diagnosis of pain origin and possible methods of treatments for pain relief in PD is of great importance. The symptoms have a great negative impact on health-related quality of life. Separating PD-related pain from pain of other origins is an important challenge and can be characterized as "many syndromes under the same umbrella". Among the different forms of PD-related pain, musculoskeletal pain is the most common form, accounting for 40%-90% of reported pain in PD patients. Augmentation by pathophysiological pathways other than those secondary to rigidity, tremor, or any of the other motor manifestations of the disease seems most probable. In PD, the basal ganglia process somatosensory information differently, and increased subjective pain sensitivity with lower electrical and heat-pain thresholds has been reported in PD patients. The mechanism is assumed to be diminished activity of the descending inhibitory control system of the basal ganglia. PD pain, like many of the nonmotor symptoms, remains underdiagnosed and, thus, poorly managed. A systematic collection of patient descriptions of type, quality, and duration of pain is, therefore, of utmost importance. Recent studies have validated new and more specific and dedicated pain scales for PD-related symptoms. Symptomatic treatments based on clinical pain classification include not only pharmacological but also nonpharmacological methods and, to some degree, invasive approaches. In the clinic, pharmacological and nonpharmacological interventions can be effective to varying degrees - as single therapies or in combination - and should be employed, because no therapeutic strategies have been validated to date for managing PD pain. Multimodal approaches should always be considered, dopamine replacement therapies should be adjusted, and analgesics and/or antidepressants should be considered, including the use of different forms of complementary therapies.
Keywords: Parkinson’s disease; basal ganglia; complementary therapies; nonmotor symptoms; pain; quality of life.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Nonmotor Symptoms and Natural History of Parkinson's Disease: Evidence From Cognitive Dysfunction and Role of Noninvasive Interventions.Int Rev Neurobiol. 2017;133:389-415. doi: 10.1016/bs.irn.2017.05.031. Epub 2017 Jul 13. Int Rev Neurobiol. 2017. PMID: 28802926 Review.
-
Chronic Pain Treatment Strategies in Parkinson's Disease.Neurol Int. 2020 Nov 18;12(3):61-76. doi: 10.3390/neurolint12030014. Neurol Int. 2020. PMID: 33218135 Free PMC article. Review.
-
Pain in Parkinson's disease.Mov Disord. 2012 Apr;27(4):485-91. doi: 10.1002/mds.23959. Epub 2011 Sep 23. Mov Disord. 2012. PMID: 21953990 Review.
-
Parkinson's disease patients' subjective descriptions of characteristics of chronic pain, sleeping patterns and health-related quality of life.Neuropsychiatr Dis Treat. 2012;8:435-42. doi: 10.2147/NDT.S34882. Epub 2012 Oct 12. Neuropsychiatr Dis Treat. 2012. PMID: 23091387 Free PMC article.
-
[Neuropsychiatric manifestations in Parkinson's disease].Psychiatriki. 2015 Apr-Jun;26(2):116-30. Psychiatriki. 2015. PMID: 26197101 Review. Greek, Modern.
Cited by
-
Management of Pain in Parkinson's Disease.J Parkinsons Dis. 2020;10(s1):S37-S48. doi: 10.3233/JPD-202069. J Parkinsons Dis. 2020. PMID: 32568113 Free PMC article. Review.
-
Cognitive Influences in Parkinson's Disease Patients and Their Caregivers: Perspectives From an Australian Cohort.Front Neurol. 2021 Nov 15;12:673816. doi: 10.3389/fneur.2021.673816. eCollection 2021. Front Neurol. 2021. PMID: 34867699 Free PMC article.
-
Music Therapy and Music-Based Interventions for Movement Disorders.Curr Neurol Neurosci Rep. 2019 Nov 13;19(11):83. doi: 10.1007/s11910-019-1005-0. Curr Neurol Neurosci Rep. 2019. PMID: 31720865 Review.
-
Motor Cortex Stimulation Reversed Hypernociception, Increased Serotonin in Raphe Neurons, and Caused Inhibition of Spinal Astrocytes in a Parkinson's Disease Rat Model.Cells. 2021 May 11;10(5):1158. doi: 10.3390/cells10051158. Cells. 2021. PMID: 34064617 Free PMC article.
-
Safety and tolerability of long-term apomorphine infusion in advanced Parkinson's disease: an Indian multi-center (APO-IND) experience.Sci Rep. 2023 Oct 31;13(1):18681. doi: 10.1038/s41598-023-46003-4. Sci Rep. 2023. PMID: 37907679 Free PMC article.
References
-
- Parkinson J. An essay on the shaking palsy. 1817. J Neuropsychiatry Clin Neurosci. 2002;14(2):223–236. discussion 222. - PubMed
-
- von Campenhausen S, Bornschein B, Wick R, et al. Prevalence and incidence of Parkinson’s disease in Europe. Eur Neuropsychopharmacol. 2005;15(4):473–490. - PubMed
-
- Parkinson’s Disease Foundation [webpage on the internet] Parkinson’s Disease Foundation, Inc. updated ©2016. [Accessed January 2016]. Available from: http://www.pdf.org/en/parkinson_statistics.
-
- Brooks DJ. Parkinson’s disease: diagnosis. Parkinsonism Relat Disord. 2012;18(suppl 1):S31–S33. - PubMed
-
- Negre-Pages L, Regragui W, Rascol O, DoPaMiP Study Group Chronic pain in Parkinson’s disease: the cross-sectional French DoPaMiP survey. Mov Disord. 2008;23(10):1361–1369. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
