

Functional Outcomes After Double-Row Versus Single-Row Rotator Cuff Repair: A Prospective Randomized Trial
- PMID: 27757408
- PMCID: PMC5051628
- DOI: 10.1177/2325967116667398
Functional Outcomes After Double-Row Versus Single-Row Rotator Cuff Repair: A Prospective Randomized Trial
Abstract
Background: The functional benefits of double-row (DR) versus single-row (SR) rotator cuff repair are not clearly established.
Purpose: To examine the effect of DR versus SR rotator cuff repair on functional outcomes and strength recovery in patients with full-thickness tears.
Study design: Randomized controlled trial; Level of evidence, 2.
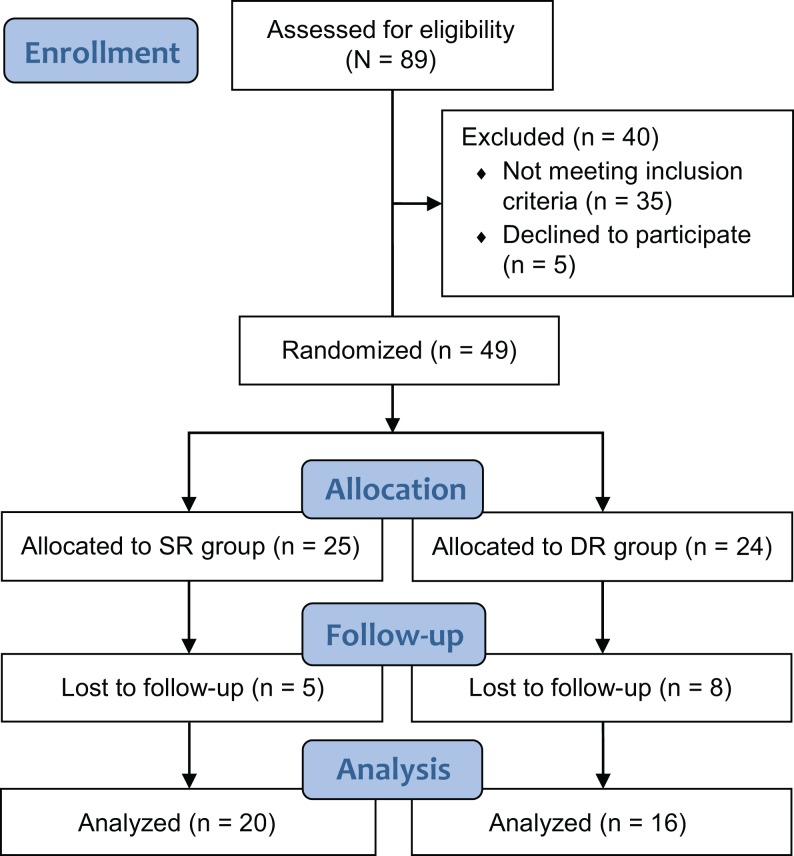
Methods: Forty-nine patients were randomized to DR or SR repairs; 36 patients (13 women, 23 men; mean age, 62 ± 7 years; 20 SR, 16 DR) were assessed at a mean 2.2 ± 1.6 years after surgery (range, 1-7 years; tear size: 17 medium, 13 large, 9 massive). The following data were recorded prior to surgery and at follow-up: Penn shoulder score, American Shoulder and Elbow Surgeons (ASES), and Simple Shoulder Test (SST) results; range of motion (ROM) for shoulder flexion, external rotation (ER) at 0° and 90° of abduction, and internal rotation (IR) at 90° of abduction; and shoulder strength (Lafayette manual muscle tester) in empty- and full-can tests, abduction, and ER at 0° of abduction. Treatment (SR vs DR) × time (pre- vs postoperative) mixed-model analysis of variance was used to assess the effect of rotator cuff repair.
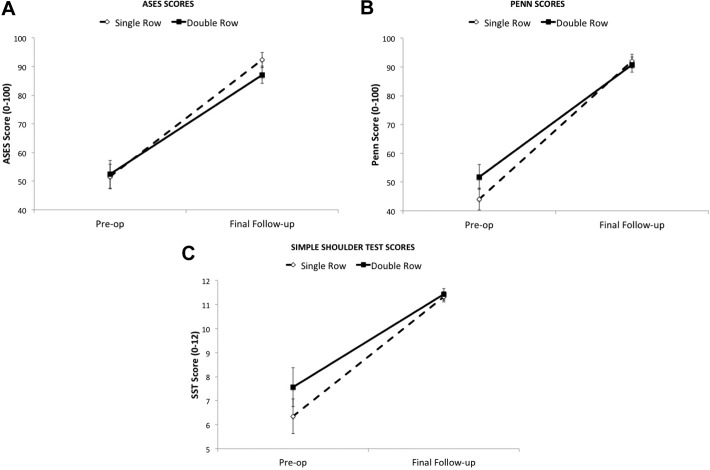
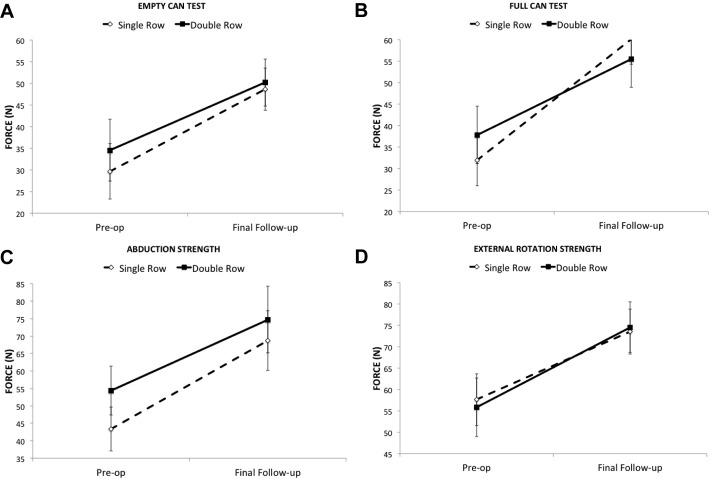
Results: Rotator cuff repair markedly improved Penn, ASES, and SST scores (P < .001), with similar improvement between SR and DR repairs (treatment × time, P = .38-.10) and excellent scores at follow-up (DR vs SR: Penn, 91 ± 11 vs 92 ± 11 [P = .73]; ASES, 87 ± 12 vs 92 ± 12 [P = .21]; SST, 11.4 ± 1.0 vs 11.3 ± 1.0 [P = .76]). Patients with DR repairs lost ER ROM at 0° of abduction (preoperative to final follow-up, 7° ± 10° loss [P = .013]). ER ROM did not significantly change with SR repair (5° ± 14° gain, P = .16; treatment by time, P = .008). This effect was not apparent for ER ROM at 90° of abduction (treatment × time, P = .26). IR ROM improved from preoperative to final follow-up (P < .01; SR, 17° ± 27°; DR, 7° ± 21°; treatment × time, P = .23). Rotator cuff repair markedly improved strength in empty-can (54%), full-can (66%), abduction (47%), and ER (54%) strength (all P < .001), with no difference between SR and DR repairs (P = .23-.75). All clinical tests with the exception of the lift-off test were normalized at follow-up (P < .05).
Conclusion: Outcomes were not different between SR or DR repair, with generally excellent outcomes for both groups. Rotator cuff repair and subsequent rehabilitation markedly improved shoulder strength.
Keywords: empty-can test; full-thickness tear; handheld dynamometer; shoulder strength.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. receives royalties from Arthrex Inc. S.J.L. is a paid consultant for Arthrex Inc.
Figures
References
-
- Aydin N, Kocaoglu B, Guven O. Single-row versus double-row arthroscopic rotator cuff repair in small- to medium-sized tears. J Shoulder Elbow Surg. 2010;19:722–725. - PubMed
-
- Burks RT, Crim J, Brown N, Fink B, Greis PE. A prospective randomized clinical trial comparing arthroscopic single- and double-row rotator cuff repair: magnetic resonance imaging and early clinical evaluation. Am J Sports Med. 2009;37:674–682. - PubMed
-
- Chen M, Xu W, Dong Q, Huang Q, Xie Z, Mao Y. Outcomes of single-row versus double-row arthroscopic rotator cuff repair: a systematic review and meta-analysis of current evidence. Arthroscopy. 2013;29:1437–1449. - PubMed
-
- Dahm DL. Controversy remains regarding the optimal technique for arthroscopic rotator cuff repair. J Bone Joint Surg Am. 2012;94:106. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
