

Advantages and disadvantages of posterolateral approach for percutaneous endoscopic lumbar discectomy
- PMID: 27757427
- PMCID: PMC5067274
- DOI: 10.21037/jss.2016.09.03
Advantages and disadvantages of posterolateral approach for percutaneous endoscopic lumbar discectomy
Abstract
Background: Percutaneous endoscopic lumbar discectomy (PELD) is one of the less invasive treatments for lumbar disc herniation (LDH), and has 3 different operative approaches. This study focused on the posterolateral approach (PLA) and investigated the appropriate operative indication.
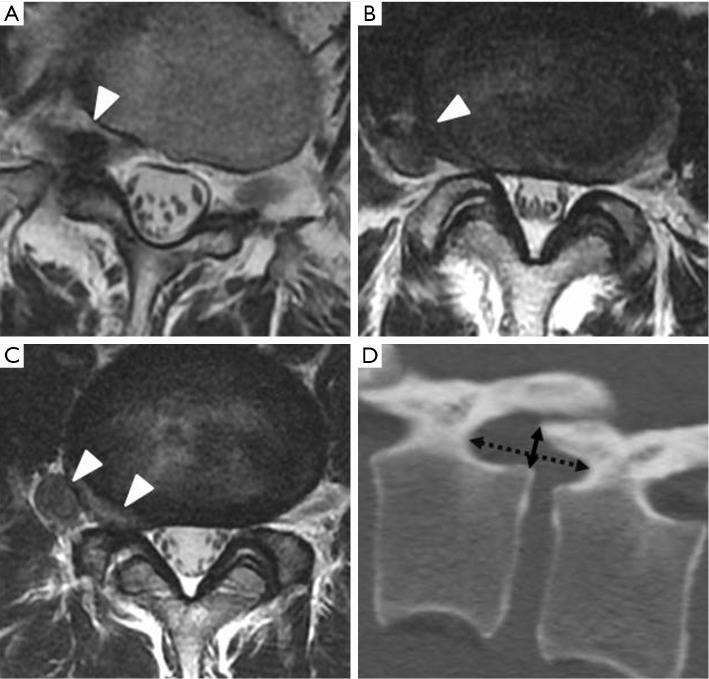
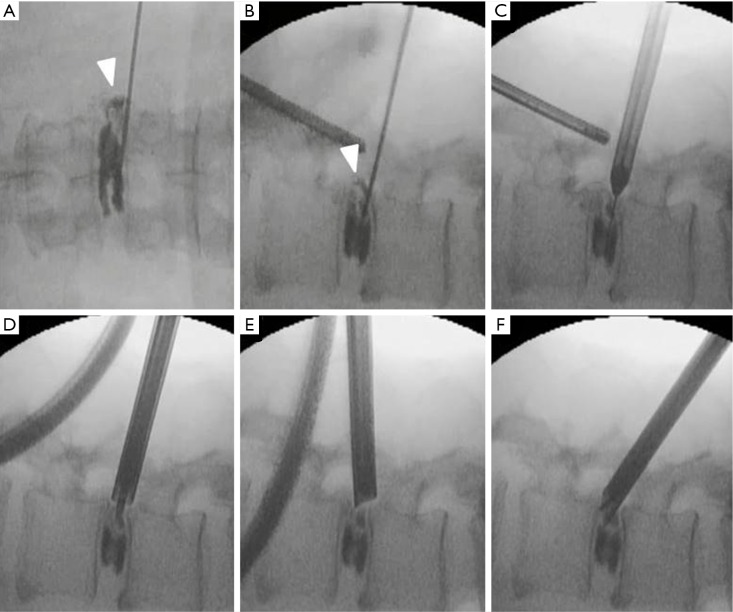
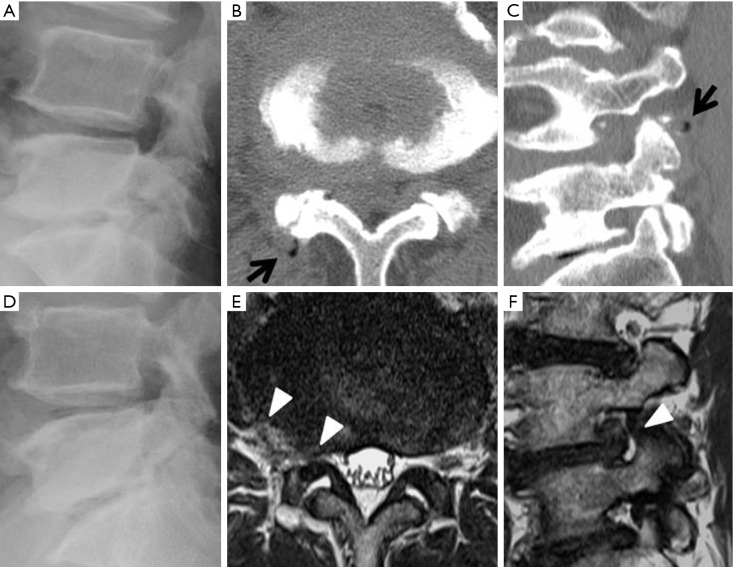
Methods: PLA was performed in 29 patients with foraminal and extraforaminal LDH. The height and width of the foramen, LDH type, and positional relationship between LDH and the foramen were radiologically evaluated. Foraminoplasty was also performed in 12 cases including those combined with intra-canal LDH or osseous foraminal stenosis. Pre- and postoperative status was evaluated using Numerical Rating Scale (NRS) scores.
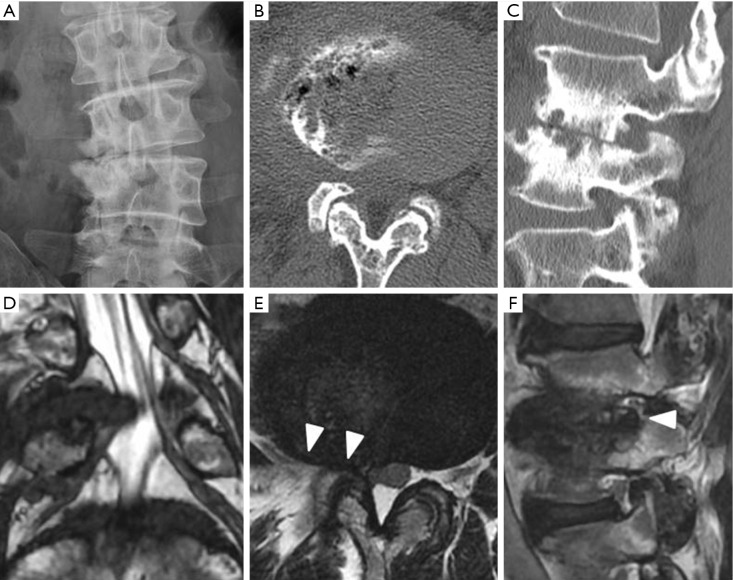
Results: Patient mean age was 56.8 years; there was single-level involvement at L3/4 (13 cases) and at L4/5 (13 cases). The mean pre- and postoperative NRS scores were 6.1 and 1.8, respectively. Early recurrence developed in a patient who was found to have local scoliosis at the corresponding vertebral level.
Conclusions: PLA can be safely used to treat foraminal and extraforaminal LDH with foraminal height ≥13 mm and foraminal width ≥7 mm. The procedure is effective for preserving the facet joint; however, we should carefully consider the indications when local scoliosis and/or instability are present.
Keywords: Percutaneous endoscopic lumbar discectomy (PELD); foraminoplasty; lumbar disc herniation (LDH); minimally invasive; posterolateral approach.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Consideration of proper operative route for interlaminar approach for percutaneous endoscopic lumbar discectomy.J Spine Surg. 2016 Dec;2(4):281-288. doi: 10.21037/jss.2016.11.05. J Spine Surg. 2016. PMID: 28097245 Free PMC article.
-
Percutaneous Endoscopic Transforaminal Outside-In Outside Technique for Foraminal and Extraforaminal Lumbar Disc Herniations-Operative Technique.World Neurosurg. 2019 Oct;130:244-253. doi: 10.1016/j.wneu.2019.07.005. Epub 2019 Jul 9. World Neurosurg. 2019. PMID: 31299304
-
The Evolution and Advancement of Endoscopic Foraminal Surgery: One Surgeon's Experience Incorporating Adjunctive Techologies.SAS J. 2007 Aug 1;1(3):108-17. doi: 10.1016/SASJ-2006-0014-RR. eCollection 2007. SAS J. 2007. PMID: 25802587 Free PMC article.
-
Comparison of percutaneous endoscopic lumbar discectomy versus microendoscopic discectomy for the treatment of lumbar disc herniation: a meta-analysis.Int Orthop. 2019 Apr;43(4):923-937. doi: 10.1007/s00264-018-4253-8. Epub 2018 Dec 13. Int Orthop. 2019. PMID: 30547214
-
Percutaneous Endoscopic Lumbar Discectomy: Indications and Complications.Pain Physician. 2020 Jan;23(1):49-56. Pain Physician. 2020. PMID: 32013278 Review.
Cited by
-
Comparison of the Outcomes of Microendoscopic Discectomy Versus Full-Endoscopic Discectomy for the Treatment of L4/5 Lumbar Disc Herniation.Global Spine J. 2024 Apr;14(3):922-929. doi: 10.1177/21925682221127997. Epub 2022 Sep 22. Global Spine J. 2024. PMID: 36134544 Free PMC article.
-
Endoscopic lumbar discectomy and minimally invasive lumbar interbody fusion: a contrastive review.Wideochir Inne Tech Maloinwazyjne. 2018 Dec;13(4):429-434. doi: 10.5114/wiitm.2018.77744. Epub 2018 Aug 22. Wideochir Inne Tech Maloinwazyjne. 2018. PMID: 30524611 Free PMC article. Review.
-
The modified transforaminal endoscopic technique in treating intracanalicular combining foraminal and/or extraforaminal lumbar disc herniations.Quant Imaging Med Surg. 2018 Oct;8(9):936-945. doi: 10.21037/qims.2018.10.02. Quant Imaging Med Surg. 2018. PMID: 30505722 Free PMC article.
-
Outcomes of epidural steroids following percutaneous transforaminal endoscopic discectomy: a meta-analysis and systematic review.Korean J Pain. 2022 Jan 1;35(1):97-105. doi: 10.3344/kjp.2022.35.1.97. Korean J Pain. 2022. PMID: 34966016 Free PMC article.
-
Full-Endoscopic Lumbar Interbody Fusion for Treating Lumbar Disc Degeneration Involving Disc Height Loss: Technical Report.Medicina (Kaunas). 2020 Sep 17;56(9):478. doi: 10.3390/medicina56090478. Medicina (Kaunas). 2020. PMID: 32957721 Free PMC article.
References
-
- Choi G, Lee SH, Deshpande K, et al. Working channel endoscope in lumbar spine surgery. J Neurosurg Sci 2014;58:77-85. - PubMed
-
- Kambin P, Sampson S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin Orthop Relat Res 1986;(207):37-43. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources