

Comprehensive First-Line Magnetic Resonance Imaging in Hypertension: Experience From a Single-Center Tertiary Referral Clinic
- PMID: 27759186
- PMCID: PMC8031106
- DOI: 10.1111/jch.12920
Comprehensive First-Line Magnetic Resonance Imaging in Hypertension: Experience From a Single-Center Tertiary Referral Clinic
Abstract
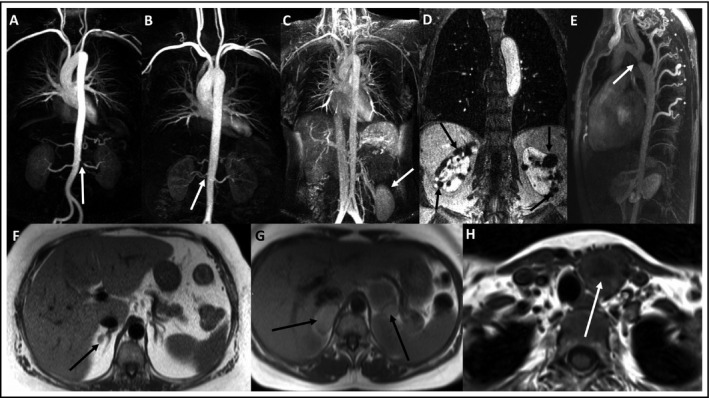
European guidelines recommend that patients with hypertension be assessed for asymptomatic organ damage and secondary causes. The authors propose that a single magnetic resonance imaging (MRI) scan can provide comprehensive first-line imaging of patients assessed via a specialist hypertension clinic. A total of 200 patients (56% male, aged 51±15 years, office BP 168±30/96±16 mm Hg) underwent MRI of the heart, kidneys, renal arteries, adrenals and aorta. Comparisons were made with other imaging modalities where available. A total of 61% had left ventricular hypertrophy (LVH), 14% had reduced ejection fraction, and 15 patients had myocardial infarcts. Echocardiography overdiagnosed LVH in 15% of patients and missed LVH in 14%. Secondary causes were identified in 14.5% of patients: 12 adrenal masses, 10 renal artery stenoses, seven thyroid abnormalities, one aortic coarctation, one enlarged pituitary gland, one polycystic kidney disease, and one renal coloboma syndrome. This comprehensive MRI protocol is an effective method of screening for asymptomatic organ damage and secondary causes of hypertension.
©2016 Wiley Periodicals, Inc.
Figures

Comment in
-
Whole-Body Imaging Procedures in Resistant Hypertension: Evaluating for Secondary Causes or to Define End-Organ Damages?J Clin Hypertens (Greenwich). 2017 Jan;19(1):23-25. doi: 10.1111/jch.12918. Epub 2016 Oct 19. J Clin Hypertens (Greenwich). 2017. PMID: 27759182 Free PMC article. No abstract available.
-
Comment on: "Comprehensive first-line magnetic resonance imaging in hypertension: experience from a single-center tertiary referral clinic".J Clin Hypertens (Greenwich). 2017 Jul;19(7):677. doi: 10.1111/jch.13027. Epub 2017 May 11. J Clin Hypertens (Greenwich). 2017. PMID: 28493420 Free PMC article. No abstract available.
References
-
- Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. - PubMed
-
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34:2159–2219. - PubMed
-
- National Clinical Guideline CG127 . Hypertension in adults: diagnosis and management. National Institute for Health and Clinical Excellence. 2011. https://www.nice.org.uk/guidance/cg127. Accessed September 28, 2016.
-
- Myerson SG, Bellenger NG, Pennell DJ. Assessment of left ventricular mass by cardiovascular magnetic resonance. Hypertension. 2002;39:750–755. - PubMed
-
- Maceira AM, Prasad SK, Pennell DJ, Mohiaddin RH. Integrated evaluation of hypertensive patients with cardiovascular magnetic resonance. Int J Cardiol. 2008;125:383–390. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
