

Lauren Histologic Type Is the Most Important Factor Associated With Pattern of Recurrence Following Resection of Gastric Adenocarcinoma
- PMID: 27759618
- PMCID: PMC5515689
- DOI: 10.1097/SLA.0000000000002040
Lauren Histologic Type Is the Most Important Factor Associated With Pattern of Recurrence Following Resection of Gastric Adenocarcinoma
Abstract
Objective: To examine sites of initial recurrence in patients after resection of gastric and gastroesophageal junction Siewert II/III adenocarcinoma (GA).
Background: There are few recent studies on recurrence for Western patients following potentially curative resection of GA.
Methods: A review of a prospectively maintained, single institution database was performed. Clinicopathologic factors, site(s) of initial recurrence, disease-free survival, and overall survival were examined.
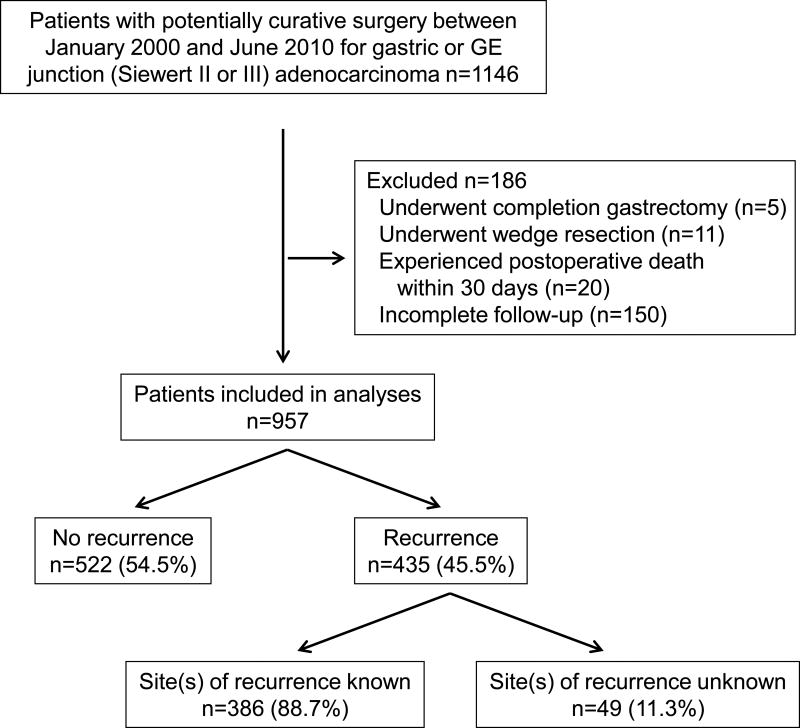
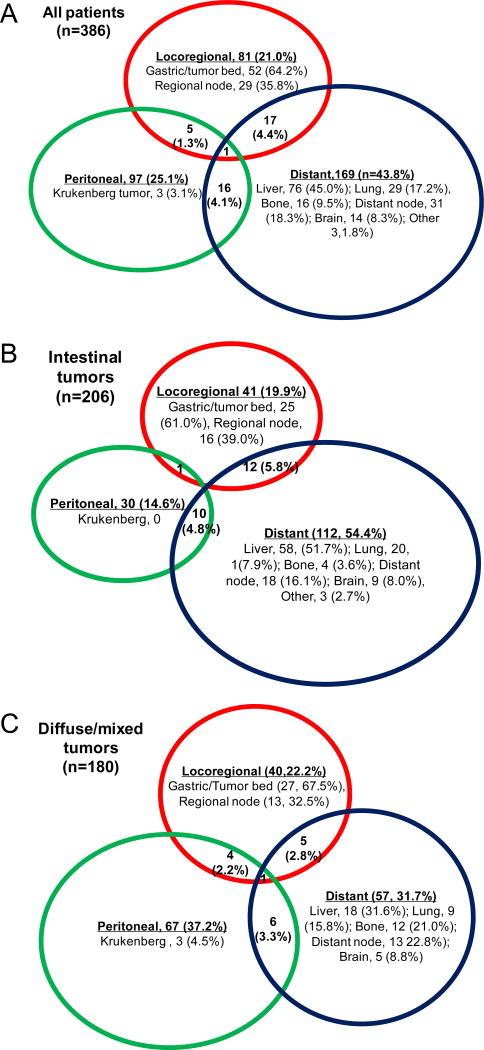
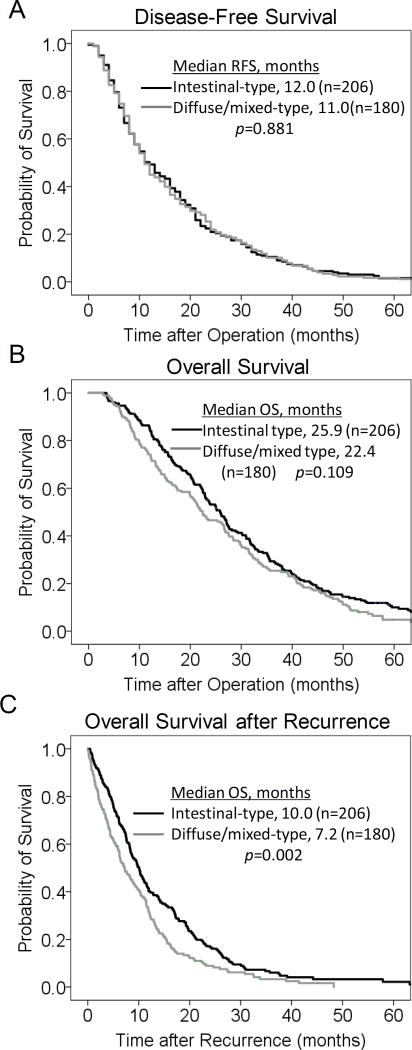
Results: From January 2000 to June 2010, 957 patients underwent potentially curative resection for GA, 435 patients (46%) had recurrent disease, and complete data on recurrence site(s) could be obtained in 386 patients. Tumors were Lauren intestinal type in 206 (53%) and diffuse or mixed-type in 180 (47%). Median time to recurrence was 12 months and 75% of recurrences occurred within 2 years. There was a significant difference in pattern of initial recurrence between the intestinal and diffuse/mixed cohorts (P < 0.001). For intestinal tumors, distant metastasis was the most common site (54%), followed by locoregional (20%), peritoneal (15%), and multifocal (11%). For diffuse/mixed tumors, peritoneal recurrence was the most common (37%), followed by distant (32%), locoregional (22%), and multifocal (9%). On multivariate analysis, Lauren histologic type was the only significant factor that was associated with both peritoneal recurrence (diffuse, hazard ratio 2.22, confidence interval 1.38-3.94) and distant recurrence (intestinal, hazard ratio 1.888, confidence interval 1.202-2.966). After recurrence, median overall survival was only 8.4 months.
Conclusions: In GA patients who recur after resection, patterns of recurrence vary significantly based on Lauren histologic type.
Conflict of interest statement
Conflict of interest: The authors declare they have no conflicts of interest.
Figures
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Bang YJ, Kim YW, Yang HK, et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet. 2012;379:315–321. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11–20. - PubMed
-
- Macdonald JS, Smalley SR, Benedetti J, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med. 2001;345:725–730. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
