

Septic Pulmonary Embolism Requiring Critical Care: Clinicoradiological Spectrum, Causative Pathogens and Outcomes
- PMID: 27759843
- PMCID: PMC5054769
- DOI: 10.6061/clinics/2016(10)02
Septic Pulmonary Embolism Requiring Critical Care: Clinicoradiological Spectrum, Causative Pathogens and Outcomes
Abstract
Objectives:: Septic pulmonary embolism is an uncommon but life-threatening disorder. However, data on patients with septic pulmonary embolism who require critical care have not been well reported. This study elucidated the clinicoradiological spectrum, causative pathogens and outcomes of septic pulmonary embolism in patients requiring critical care.
Methods:: The electronic medical records of 20 patients with septic pulmonary embolism who required intensive care unit admission between January 2005 and December 2013 were reviewed.
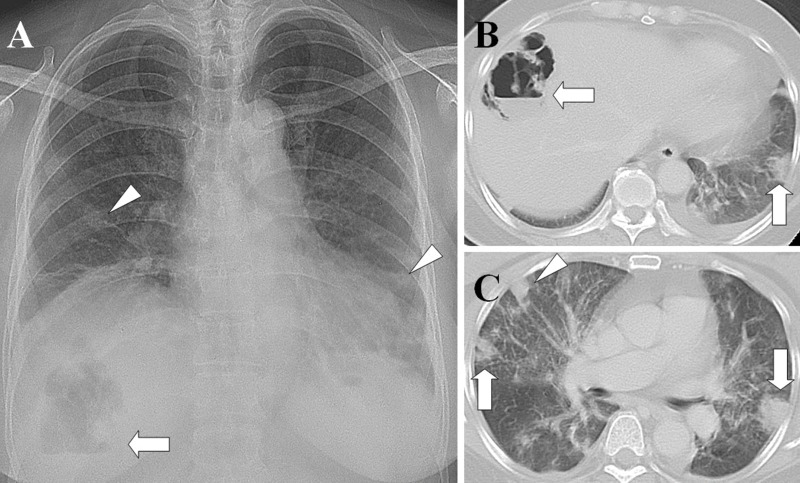
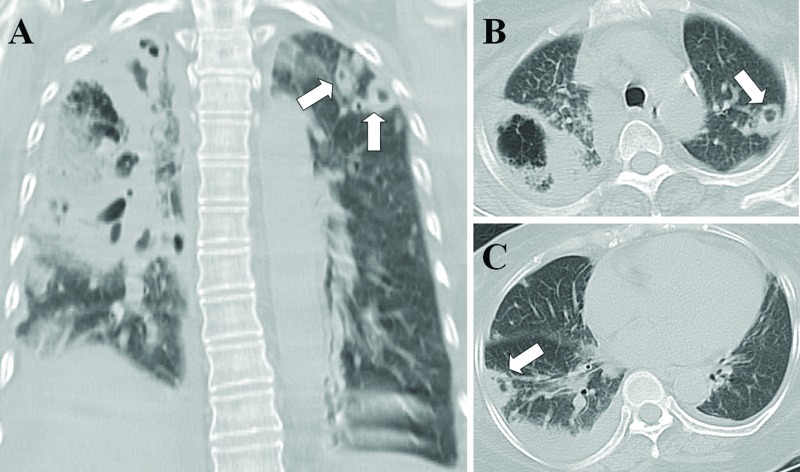
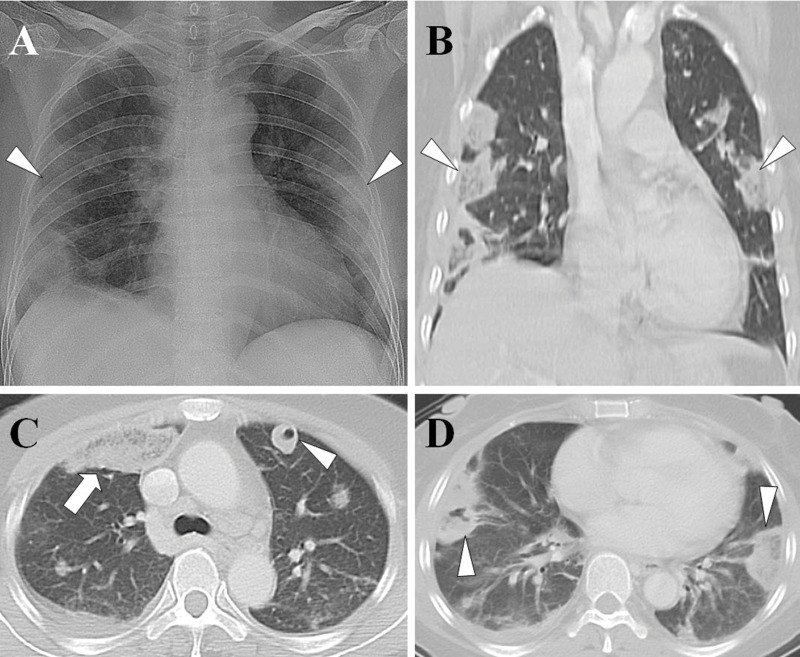
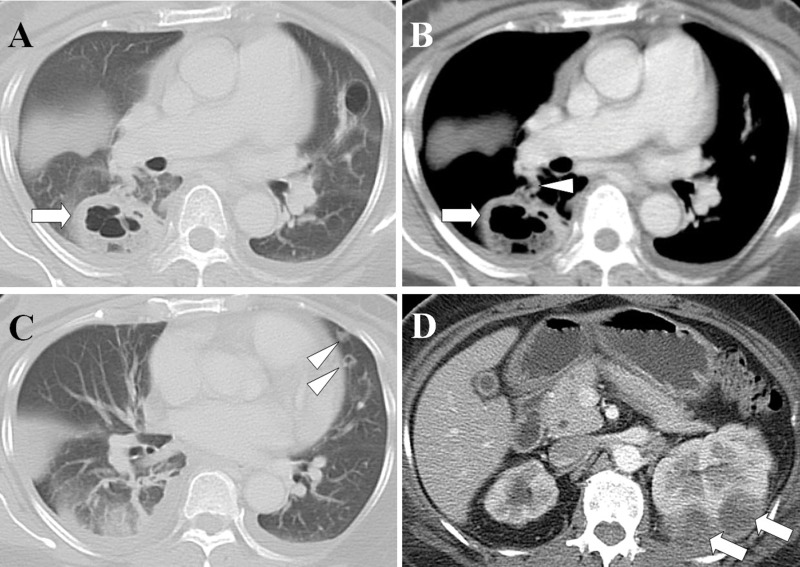
Results:: Multiple organ dysfunction syndrome developed in 85% of the patients, and acute respiratory failure was the most common organ failure (75%). The most common computed tomographic findings included a feeding vessel sign (90%), peripheral nodules without cavities (80%) or with cavities (65%), and peripheral wedge-shaped opacities (75%). The most common primary source of infection was liver abscess (40%), followed by pneumonia (25%). The two most frequent causative pathogens were Klebsiella pneumoniae (50%) and Staphylococcus aureus (35%). Compared with survivors, nonsurvivors had significantly higher serum creatinine, arterial partial pressure of carbon dioxide, and Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment scores, and they were significantly more likely to have acute kidney injury, disseminated intravascular coagulation and lung abscesses. The in-hospital mortality rate was 30%. Pneumonia was the most common cause of death, followed by liver abscess.
Conclusions:: Patients with septic pulmonary embolism who require critical care, especially those with pneumonia and liver abscess, are associated with high mortality. Early diagnosis, appropriate antibiotic therapy, surgical intervention and respiratory support are essential.
Conflict of interest statement
No potential conflict of interest was reported.
Figures
Similar articles
-
Septic pulmonary embolism caused by a Klebsiella pneumoniae liver abscess: clinical characteristics, imaging findings, and clinical courses.Clinics (Sao Paulo). 2015 Jun;70(6):400-7. doi: 10.6061/clinics/2015(06)03. Epub 2015 Jun 1. Clinics (Sao Paulo). 2015. PMID: 26106957 Free PMC article.
-
Septic pulmonary embolism in China: clinical features and analysis of prognostic factors for mortality in 98 cases.BMC Infect Dis. 2019 Dec 27;19(1):1082. doi: 10.1186/s12879-019-4672-1. BMC Infect Dis. 2019. PMID: 31881849 Free PMC article.
-
Klebsiella pneumoniae infection associated septic pulmonary embolism in an emergency department from east China.Ann Palliat Med. 2021 Feb;10(2):1521-1529. doi: 10.21037/apm-19-648. Epub 2020 Oct 27. Ann Palliat Med. 2021. PMID: 33183047
-
Liver abscess and Aeromonas bacteremia with septic pulmonary embolism.Intern Med. 2003 Oct;42(10):1047-9. doi: 10.2169/internalmedicine.42.1047. Intern Med. 2003. PMID: 14606725 Review.
-
Pyogenic hepatic abscess and septic pulmonary emboli associated with Klebsiella ozaenae bacteremia.South Med J. 1992 Jun;85(6):638-41. doi: 10.1097/00007611-199206000-00014. South Med J. 1992. PMID: 1604394 Review.
Cited by
-
Isolated pulmonary valve endocarditis in a pediatric patient with down syndrome.J Cardiothorac Surg. 2024 Aug 27;19(1):494. doi: 10.1186/s13019-024-03000-6. J Cardiothorac Surg. 2024. PMID: 39192361 Free PMC article.
-
Injection drug induced septic embolism-A growing concern.Radiol Case Rep. 2022 Sep 15;17(11):4345-4349. doi: 10.1016/j.radcr.2022.08.057. eCollection 2022 Nov. Radiol Case Rep. 2022. PMID: 36188073 Free PMC article.
-
Risk Factors for Pulmonary Embolism in ICU Patients: A Retrospective Cohort Study from the MIMIC-III Database.Clin Appl Thromb Hemost. 2022 Jan-Dec;28:10760296211073925. doi: 10.1177/10760296211073925. Clin Appl Thromb Hemost. 2022. PMID: 35043708 Free PMC article.
-
Nontrombotic Pulmonary Embolism: Different Etiology, Same Significant Consequences.J Pers Med. 2023 Jan 23;13(2):202. doi: 10.3390/jpm13020202. J Pers Med. 2023. PMID: 36836436 Free PMC article. Review.
-
Pleurisy secondary to nonthrombotic pulmonary emboli in a patient with intravenous drug use.Respir Med Case Rep. 2023 Jun 4;45:101884. doi: 10.1016/j.rmcr.2023.101884. eCollection 2023. Respir Med Case Rep. 2023. PMID: 37577124 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
