

A Novel Index Using Ankle Hemodynamic Parameters to Assess the Severity of Peripheral Arterial Disease: A Pilot Study
- PMID: 27760183
- PMCID: PMC5070739
- DOI: 10.1371/journal.pone.0164756
A Novel Index Using Ankle Hemodynamic Parameters to Assess the Severity of Peripheral Arterial Disease: A Pilot Study
Abstract
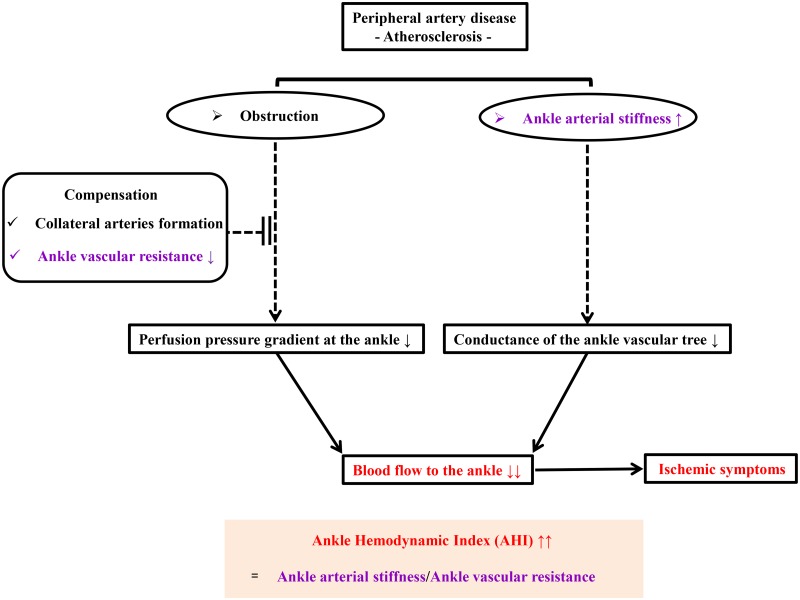
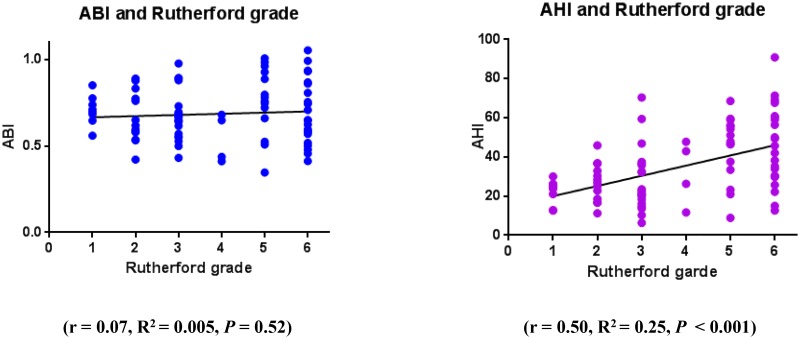
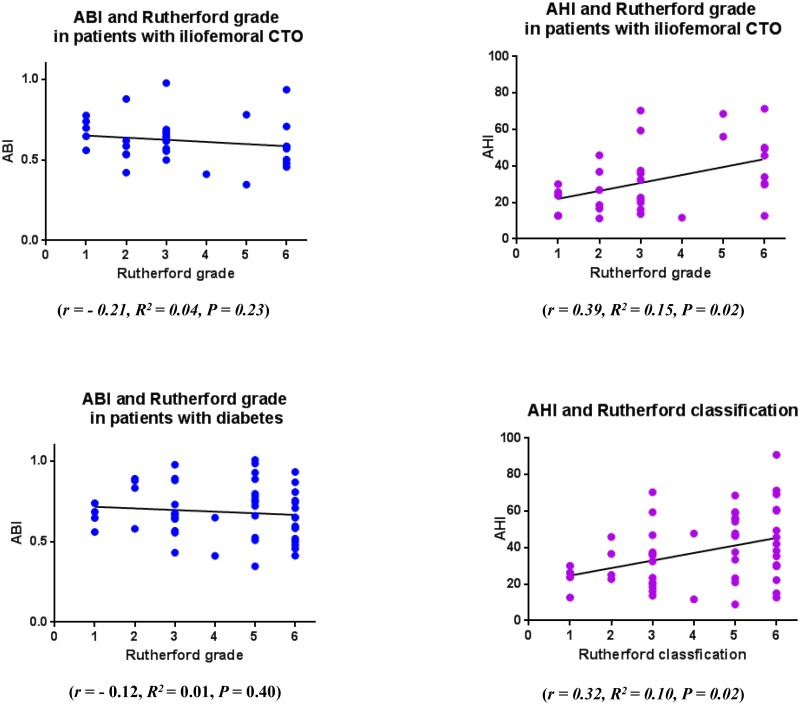
In peripheral arterial disease (PAD) of the lower extremities, the presence of flow-limiting stenoses can be objectively detected by the ankle-brachial index (ABI). However, the severity of ischemic symptoms is not necessarily associated with the ABI value. Atherosclerotic plaque in lower extremity PAD induces ankle arterial stiffness and reduces ankle vascular resistance, which may decrease ankle blood flow and cause ischemic symptoms. We hypothesized that the ankle hemodynamic index (AHI), defined as the ratio of ankle arterial stiffness to ankle vascular resistance, could be used to assess the blood supply deficiency in a diseased lower limb in patients with PAD. The 85 consecutive patients with PAD who were retrospectively analyzed in this study had Rutherford grade 1 to grade 6 ischemia diagnosed as PAD and significant stenotic lesions (>50% diameter stenosis) of the lower extremity on contrast angiography. The AHI was calculated as the product of the ankle pulse pressure and the ratio of heart rate to ankle mean arterial pressure (ankle pulse pressure × heart rate/ankle mean arterial pressure). The Rutherford grade was significantly correlated with the AHI (r = 0.50, P < 0.001), but not with the ABI (r = 0.07, P = 0.52). Multiple ordinal regression analysis showed that anemia (odds ratio 0.66, P = 0.002) and AHI (odds ratio 1.04, P = 0.02) were independently associated with Rutherford grade. Our study shows that AHI, a novel parameter based on the ABI measurement, is well correlated with ischemic symptoms, and may be a useful means to assess the arterial blood supply of the lower extremities of patients with PAD.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
An analysis of IN.PACT DEEP randomized trial on the limitations of the societal guidelines-recommended hemodynamic parameters to diagnose critical limb ischemia.J Vasc Surg. 2016 May;63(5):1311-7. doi: 10.1016/j.jvs.2015.11.042. Epub 2016 Feb 6. J Vasc Surg. 2016. PMID: 26860642 Clinical Trial.
-
Comparison of accuracy of two different methods to determine ankle-brachial index to predict peripheral arterial disease severity confirmed by angiography.Am J Cardiol. 2014 Oct 1;114(7):1105-10. doi: 10.1016/j.amjcard.2014.07.023. Epub 2014 Jul 17. Am J Cardiol. 2014. PMID: 25129876
-
The ankle--brachial index and the diabetic foot: a troublesome marriage.Ann Vasc Surg. 2011 Aug;25(6):770-7. doi: 10.1016/j.avsg.2010.12.025. Epub 2011 Apr 21. Ann Vasc Surg. 2011. PMID: 21514102
-
The toe-brachial index in the diagnosis of peripheral arterial disease.J Vasc Surg. 2013 Jul;58(1):231-8. doi: 10.1016/j.jvs.2013.03.044. Epub 2013 May 18. J Vasc Surg. 2013. PMID: 23688630 Review.
-
Characteristics of peripheral arterial disease and its relevance to the diabetic population.Int J Low Extrem Wounds. 2011 Sep;10(3):152-66. doi: 10.1177/1534734611417352. Epub 2011 Aug 19. Int J Low Extrem Wounds. 2011. PMID: 21856972 Review.
Cited by
-
Vascular resistance index and the immediate hemodynamic success of lower limb distal artery revascularization.J Vasc Bras. 2024 Mar 4;23:e20230119. doi: 10.1590/1677-5449.202301192. eCollection 2024. J Vasc Bras. 2024. PMID: 38487516 Free PMC article.
-
Correlation between the vascular resistance index and arteriography for assessment of the distal arterial bed in chronic limb threatening ischemia.J Vasc Bras. 2024 Feb 5;23:e20230071. doi: 10.1590/1677-5449.202300712. eCollection 2024. J Vasc Bras. 2024. PMID: 38433983 Free PMC article.
References
-
- Fowkes FGR, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. The Lancet. 2013;382(9901):1329–40. - PubMed
-
- Harris LM, Faggioli GL, Shah R, Koerner N, Lillis L, Dandona P, et al. Vascular reactivity in patients with peripheral vascular disease. Am J Cardiol. 1995;76(3):207–12. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
