

A Common Profile of Disordered Angiogenic Factor Production and the Exacerbation of Inflammation in Early Preeclampsia, Late Preeclampsia, and Intrauterine Growth Restriction
- PMID: 27760191
- PMCID: PMC5070778
- DOI: 10.1371/journal.pone.0165060
A Common Profile of Disordered Angiogenic Factor Production and the Exacerbation of Inflammation in Early Preeclampsia, Late Preeclampsia, and Intrauterine Growth Restriction
Abstract
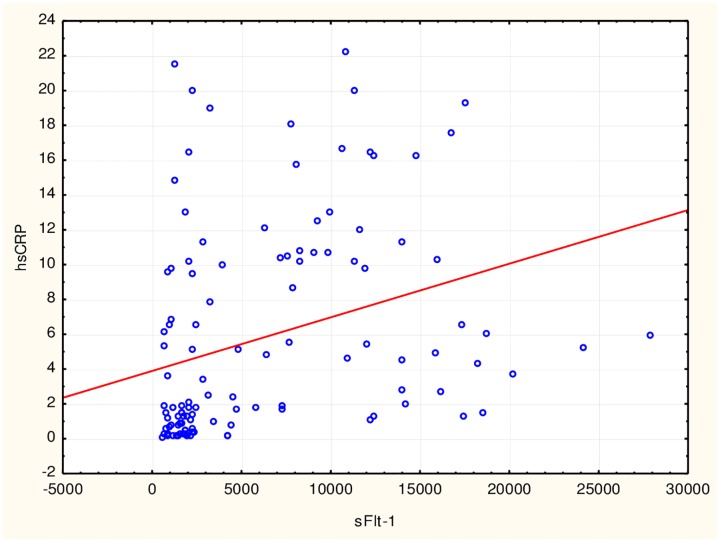
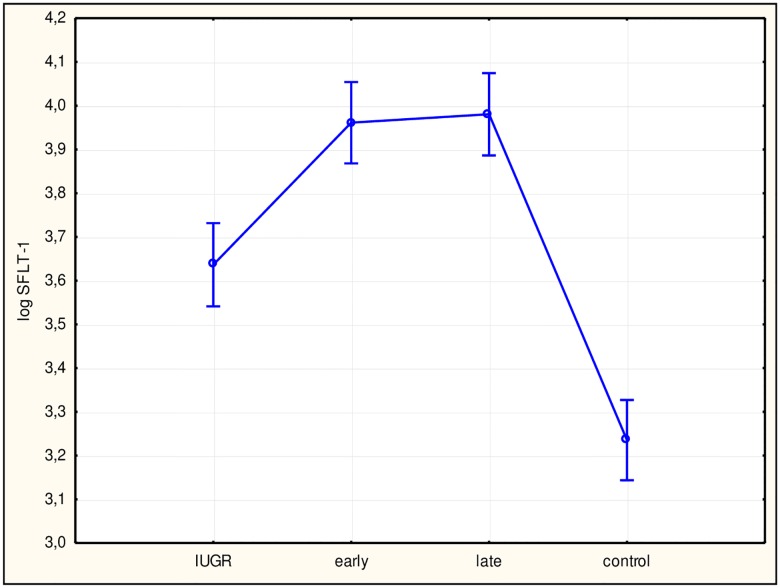
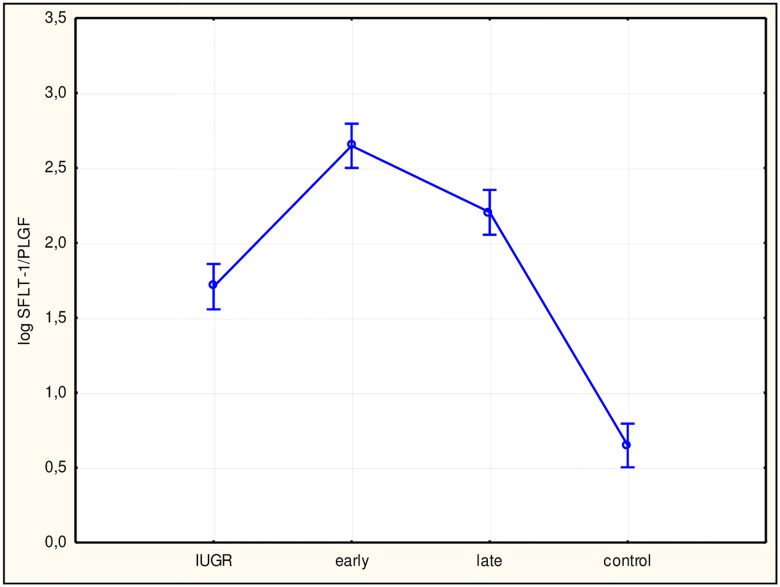
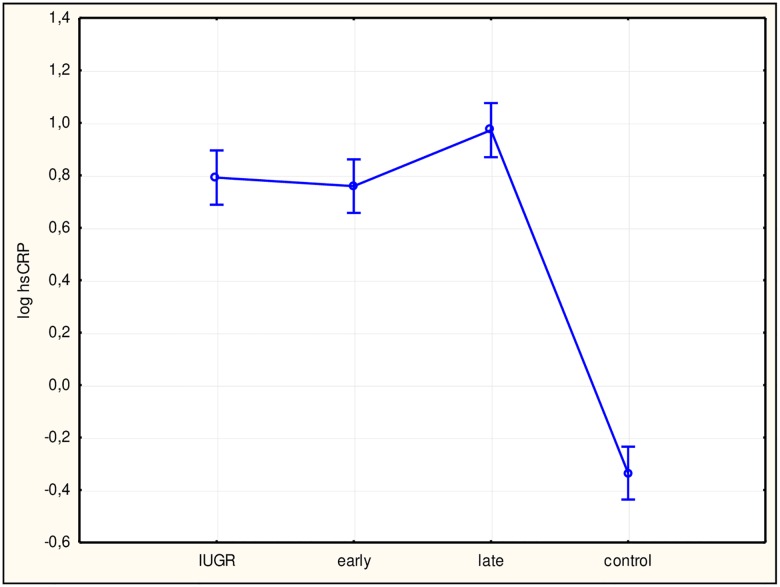
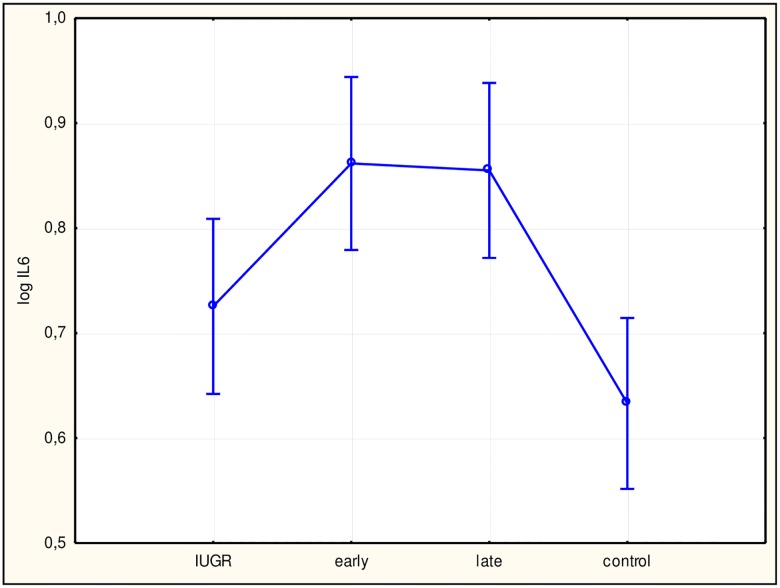
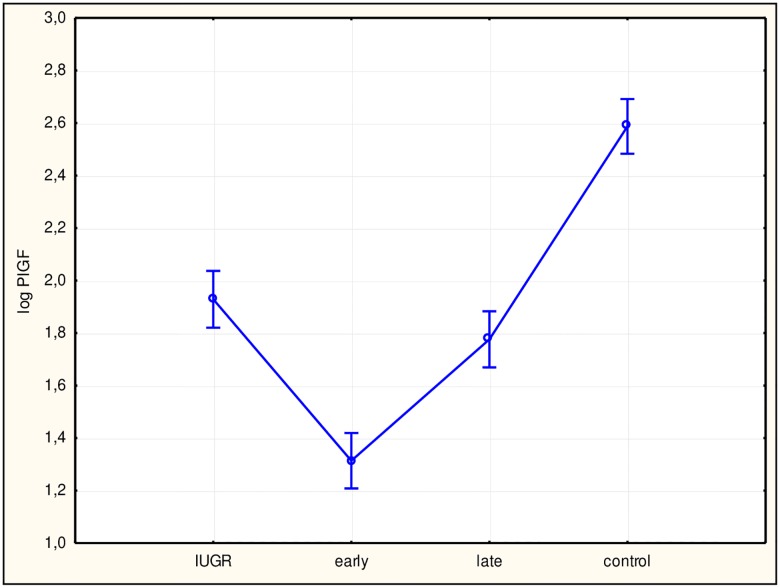
Preeclampsia and intrauterine growth restriction are two separate disease entities that, according to numerous reports, share the same pathogenesis. In both, angiogenesis disorders and generalized inflammation are the dominant symptoms. In this study, we hypothesized that both diseases demonstrate the same profile in early preeclampsia, late preeclampsia, and intrauterine growth restriction patients, with the only difference being the degree of exacerbation of lesions. One hundred sixty-seven patients were enrolled in the study and divided into four groups: early preeclampsia, late preeclampsia, and intrauterine growth restriction groups, and one control group. Concentrations of the angiogenesis and inflammatory markers soluble fms-like tyrosine kinase receptor 1, placental growth factor, high-sensitivity C-reactive protein, and interleukin-6 were determined, and the behavior of these markers and correlations among them were studied. Higher concentrations of soluble fms-like tyrosine kinase receptor 1, high-sensitivity C-reactive protein, and interleukin-6 and a lower concentration of placental growth factor were observed in the study groups compared with the control group. No differences in concentrations of the studied markers were found among the study groups but significant correlations were observed. The higher values for the angiogenesis and inflammatory markers both in preeclampsia patients and patients with intrauterine growth restriction of placental origin compared with the control group suggest the existence of the same underlying disorders in the development of these pathologies. The observed mutual correlations for disordered angiogenesis and inflammatory markers are suggestive of a mutual relationship between these processes in the development of pathologies evolving secondary to placental ischemia. The same lesion profile was observed for both preeclampsia and 'placental' intrauterine growth restriction patients, which could be used in developing common diagnostic criteria for pregnant patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Maternal endothelial damage as a disorder shared by early preeclampsia, late preeclampsia and intrauterine growth restriction.J Perinat Med. 2017 Oct 26;45(7):793-802. doi: 10.1515/jpm-2016-0178. J Perinat Med. 2017. PMID: 27865093
-
In vivo uteroplacental release of placental growth factor and soluble Fms-like tyrosine kinase-1 in normal and preeclamptic pregnancies.Am J Obstet Gynecol. 2016 Dec;215(6):782.e1-782.e9. doi: 10.1016/j.ajog.2016.07.056. Epub 2016 Aug 5. Am J Obstet Gynecol. 2016. PMID: 27503620
-
Placental angiogenic growth factors and uterine artery Doppler findings for characterization of different subsets in preeclampsia and in isolated intrauterine growth restriction.Am J Obstet Gynecol. 2006 Jul;195(1):201-7. doi: 10.1016/j.ajog.2006.01.014. Epub 2006 Mar 20. Am J Obstet Gynecol. 2006. PMID: 16545329
-
Markers for presymptomatic prediction of preeclampsia and intrauterine growth restriction.Hypertens Pregnancy. 2004;23(2):171-89. doi: 10.1081/PRG-120028292. Hypertens Pregnancy. 2004. PMID: 15369650 Review.
-
[Predictive and prognostic factors of preeclampsia: Interest of PlGF and sFLT-1].J Gynecol Obstet Biol Reprod (Paris). 2016 Nov;45(9):999-1008. doi: 10.1016/j.jgyn.2016.02.006. Epub 2016 Jul 7. J Gynecol Obstet Biol Reprod (Paris). 2016. PMID: 27212611 Review. French.
Cited by
-
Bioinformatics Analysis Identifies Potential Related Genes in the Pathogenesis of Intrauterine Fetal Growth Retardation.Evol Bioinform Online. 2022 Jul 28;18:11769343221112780. doi: 10.1177/11769343221112780. eCollection 2022. Evol Bioinform Online. 2022. PMID: 35923419 Free PMC article.
-
Inflammatory Markers in Mother's Own Milk and Infant Stool of Very Low Birthweight Infants.J Hum Lact. 2023 Nov;39(4):656-665. doi: 10.1177/08903344231192441. Epub 2023 Aug 31. J Hum Lact. 2023. PMID: 37653641 Free PMC article. Clinical Trial.
-
Placental origins of neonatal diseases: toward a precision medicine approach.Pediatr Res. 2021 Jan;89(2):377-383. doi: 10.1038/s41390-020-01293-6. Epub 2020 Dec 7. Pediatr Res. 2021. PMID: 33288874 Review.
-
The protective effects of some herbs on mitigating HFD-induced obesity via enhancing biochemical indicators and fertility in female rats.Heliyon. 2024 May 1;10(9):e30249. doi: 10.1016/j.heliyon.2024.e30249. eCollection 2024 May 15. Heliyon. 2024. PMID: 38726161 Free PMC article.
-
Regulation of Placental Development and Its Impact on Fetal Growth-New Insights From Mouse Models.Front Endocrinol (Lausanne). 2018 Sep 27;9:570. doi: 10.3389/fendo.2018.00570. eCollection 2018. Front Endocrinol (Lausanne). 2018. PMID: 30319550 Free PMC article. Review.
References
-
- Brosens IA, Robertson WB, Dixon HG. The role of spiral arteries in the pathogenesis of preeclampsia. Obset Gynecol Annu. 1972;1: 177–191. - PubMed
-
- Gerretsen GG, Huisjes HJ, Elema JD. Morphological changes of the spiral arteries in the placental bed in relation to preeclampsia and fetal growth retardation. Br J Obstet Gynaecol. 1981;88: 876–881. - PubMed
-
- Khong TY, De Wolf F, Robertson WB, Brosens I. Inadequate maternal vascular response to placentation in pregnancies complicated by pre-eclampsia and by small-for-gestational age infants. Br J Obstet Gynaecol. 1986;93: 1049–1059. - PubMed
-
- Cindrova-Davies T, Herrera EA, Niu Y, Kindom J, Giussani DA, Burton GJ. Reduced cystathionine y-lyase and increased miR-21 expression are associated with increased vascular resistance in growth-restricted pregnancies: hydrogen sulfide as a placental vasodilator. Am J Pathol. 2013;182: 1448–1458. 10.1016/j.ajpath.2013.01.001 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
