

Association of Preoperative Risk Factors With Malignancy in Pancreatic Mucinous Cystic Neoplasms: A Multicenter Study
- PMID: 27760255
- PMCID: PMC5560258
- DOI: 10.1001/jamasurg.2016.3598
Association of Preoperative Risk Factors With Malignancy in Pancreatic Mucinous Cystic Neoplasms: A Multicenter Study
Abstract
Importance: Pancreatic mucinous cystic neoplasms (MCNs) harbor malignant potential, and current guidelines recommend resection. However, data are limited on preoperative risk factors for malignancy (adenocarcinoma or high-grade dysplasia) occurring in the setting of an MCN.
Objectives: To examine the preoperative risk factors for malignancy in resected MCNs and to assess outcomes of MCN-associated adenocarcinoma.
Design, setting, and participants: Patients who underwent pancreatic resection of MCNs at the 8 academic centers of the Central Pancreas Consortium from January 1, 2000, through December 31, 2014, were retrospectively identified. Preoperative factors of patients with and without malignant tumors were compared. Survival analyses were conducted for patients with adenocarcinoma.
Main outcomes and measures: Binary logistic regression models were used to determine the association of preoperative factors with the presence of MCN-associated malignancy.
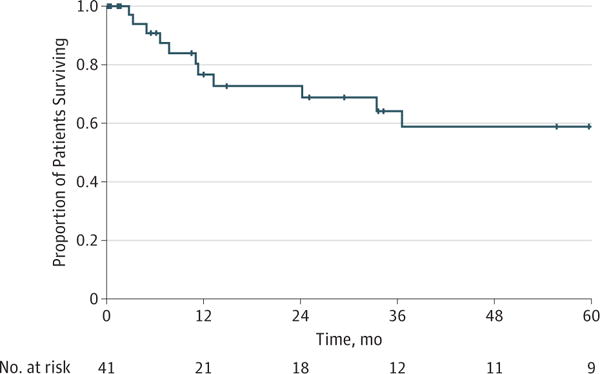
Results: A total of 1667 patients underwent resection of pancreatic cystic lesions, and 349 (20.9%) had an MCN (310 women [88.8%]; mean (SD) age, 53.3 [14.7] years). Male sex (odds ratio [OR], 3.72; 95% CI, 1.21-11.44; P = .02), pancreatic head and neck location (OR, 3.93; 95% CI, 1.43-10.81; P = .01), increased radiographic size of the MCN (OR, 1.17; 95% CI, 1.08-1.27; P < .001), presence of a solid component or mural nodule (OR, 4.54; 95% CI, 1.95-10.57; P < .001), and duct dilation (OR, 4.17; 95% CI, 1.63-10.64; P = .003) were independently associated with malignancy. Malignancy was not associated with presence of radiographic septations or preoperative cyst fluid analysis (carcinoembryonic antigen, amylase, or mucin presence). The median serum CA19-9 level for patients with malignant neoplasms was 210 vs 15 U/mL for those without (P = .001). In the 44 patients with adenocarcinoma, 41 (93.2%) had lymph nodes harvested, with nodal metastases in only 14 (34.1%). Median follow-up for patients with adenocarcinoma was 27 months. Adenocarcinoma recurred in 11 patients (25%), with a 64% recurrence-free survival and 59% overall survival at 3 years.
Conclusions and relevance: Adenocarcinoma or high-grade dysplasia is present in 14.9% of resected pancreatic MCNs for which risks include male sex, pancreatic head and neck location, larger MCN, solid component or mural nodule, and duct dilation. Mucinous cystic neoplasm-associated adenocarcinoma appears to have decreased nodal involvement at the time of resection and increased survival compared with typical pancreatic ductal adenocarcinoma. Indications for resection of MCNs should be revisited.
Conflict of interest statement
Figures

Comment in
-
A Brave New World of Research Ethics.JAMA Surg. 2017 Jan 1;152(1):9. doi: 10.1001/jamasurg.2016.3201. JAMA Surg. 2017. PMID: 27732697 No abstract available.
References
-
- Adsay NV. Cystic neoplasia of the pancreas: pathology and biology. J Gastrointest Surg. 2008;12(3):401–404. - PubMed
-
- Compagno J, Oertel JE. Microcystic adenomas of the pancreas (glycogen-rich cystadenomas): a clinicopathologic study of 34 cases. Am J Clin Pathol. 1978;69(3):289–298. - PubMed
-
- Compagno J, Oertel JE. Mucinous cystic neoplasms of the pancreas with overt and latent malignancy (cystadenocarcinoma and cystadenoma): a clinicopathologic study of 41 cases. Am J Clin Pathol. 1978;69(6):573–580. - PubMed
-
- Aaltonen LA, Hamilton SR, World Health Organization, International Agency for Research on Cancer . Pathology and Genetics of Tumours of the Digestive System. Oxford, England: Oxford University Press; 2000.
-
- Zamboni G, Klöppel G, Hruban RH, Longnecker DS, Adler G. Mucinous cystic neoplasms of the pancreas. In: Bosman FTCF, Hruban RH, editors. WHO Classification of Tumours of the Digestive System. Vol. 2010. Lyon, France: International Agency for Research on Cancer; pp. 234–236.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
