

Heated insufflation with or without humidification for laparoscopic abdominal surgery
- PMID: 27760282
- PMCID: PMC6464153
- DOI: 10.1002/14651858.CD007821.pub3
Heated insufflation with or without humidification for laparoscopic abdominal surgery
Abstract
Background: Intraoperative hypothermia during both open and laparoscopic abdominal surgery may be associated with adverse events. For laparoscopic abdominal surgery, the use of heated insufflation systems for establishing pneumoperitoneum has been described to prevent hypothermia. Humidification of the insufflated gas is also possible. Past studies on heated insufflation have shown inconclusive results with regards to maintenance of core temperature and reduction of postoperative pain and recovery times.
Objectives: To determine the effect of heated gas insufflation compared to cold gas insufflation on maintaining intraoperative normothermia as well as patient outcomes following laparoscopic abdominal surgery.
Search methods: We searched Cochrane Colorectal Cancer Specialised Register (September 2016), the Cochrane Central Register of Controlled Trials (CENTRAL; The Cochrane Library 2016, Issue 8), Ovid MEDLINE (1950 to September 2016), Ovid Embase (1974 to September 2016), International Pharmaceutical Abstracts (IPA) (September 2016), Web of Science (1985 to September 2016), Scopus, www.clinicaltrials.gov and the National Research Register (1956 to September 2016). We also searched grey literature and cross references. Searches were limited to human studies without language restriction.
Selection criteria: Only randomised controlled trials comparing heated (with or without humidification) with cold gas insufflation in adult and paediatric populations undergoing laparoscopic abdominal procedures were included. We assessed study quality in regards to relevance, design, sequence generation, allocation concealment, blinding, possibility of incomplete data and selective reporting. Two review authors independently selected studies for the review, with any disagreement resolved in consensus with a third co-author.
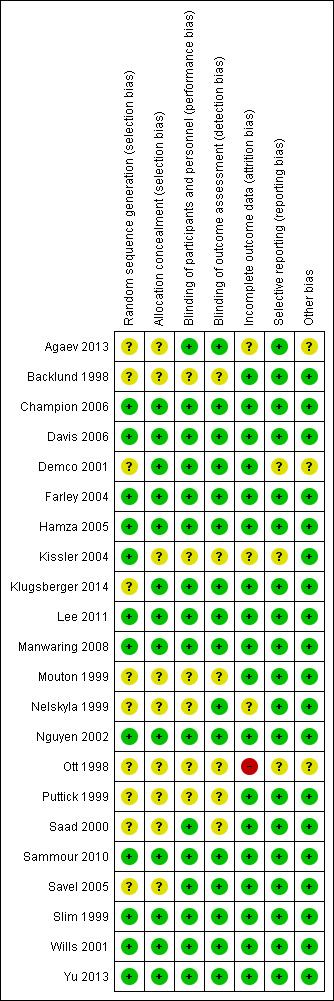
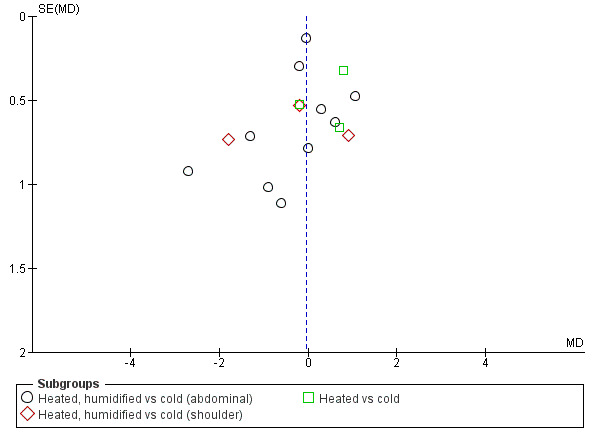
Data collection and analysis: Two review authors independently performed screening of eligible studies, data extraction and methodological quality assessment of the trials. We classified a study as low-risk of bias if all of the first six main criteria indicated in the 'Risk of Bias Assessment' table were assessed as low risk. We used data sheets to collect data from eligible studies. We presented results using mean differences for continuous outcomes and relative risks for dichotomous outcomes, with 95% confidence intervals. We used Review Manager (RevMan) 5.3 software to calculate the estimated effects. We took publication bias into consideration and compiled funnel plots.
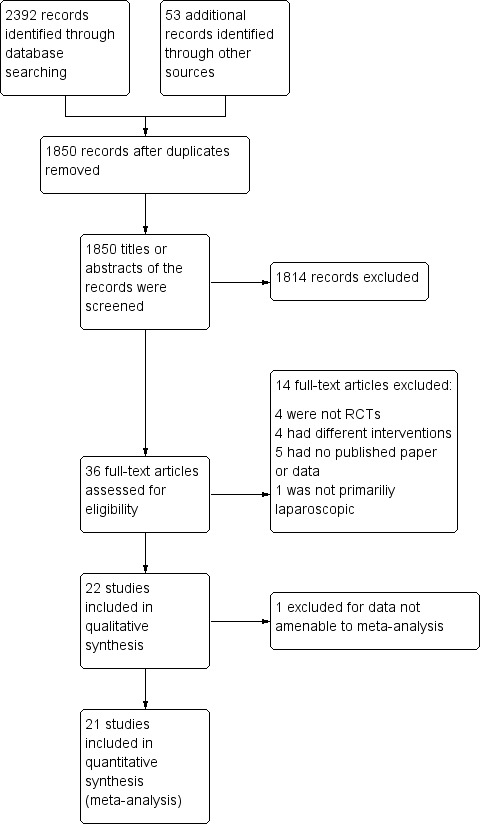
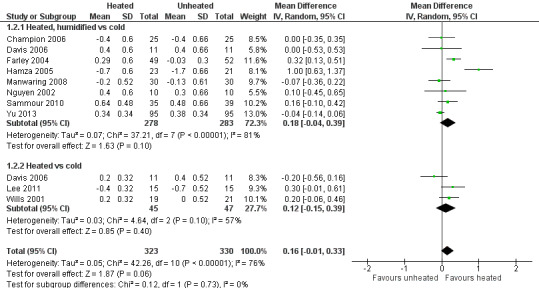
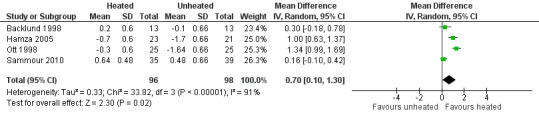
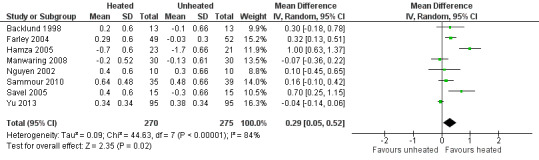
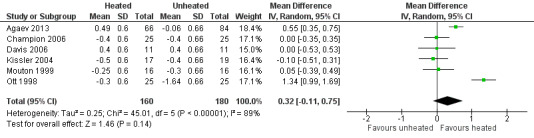
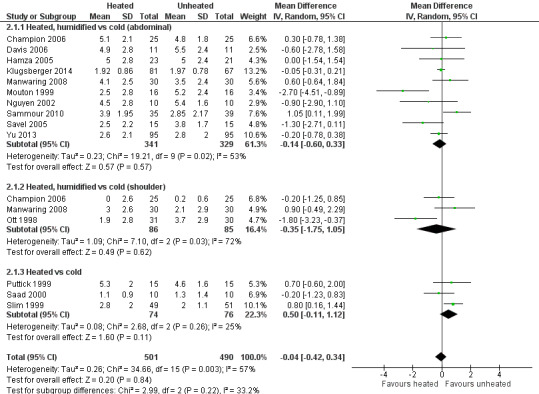
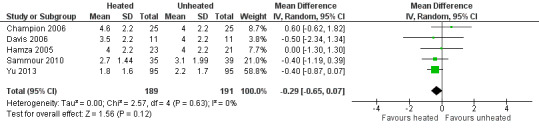
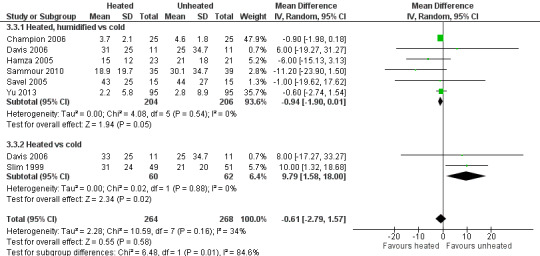
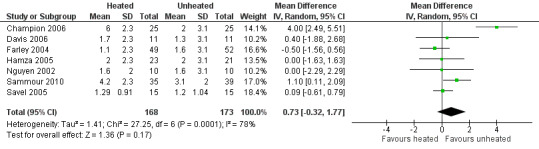
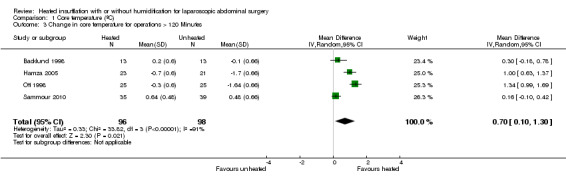
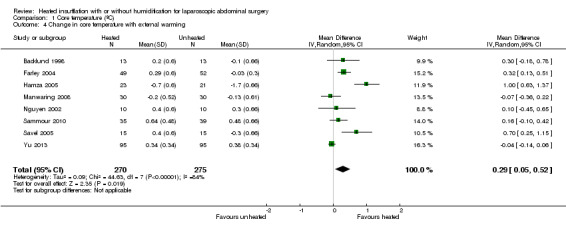
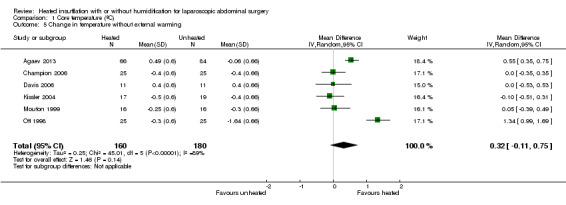
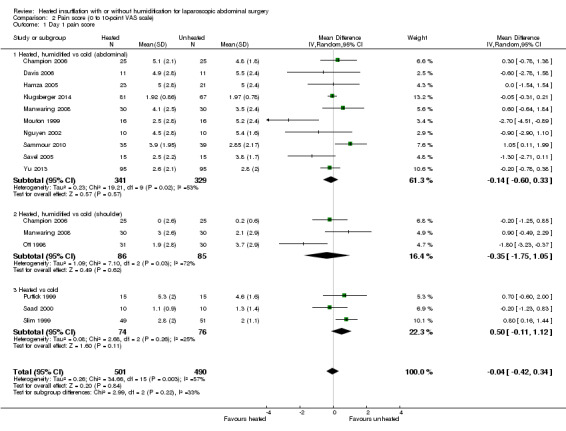
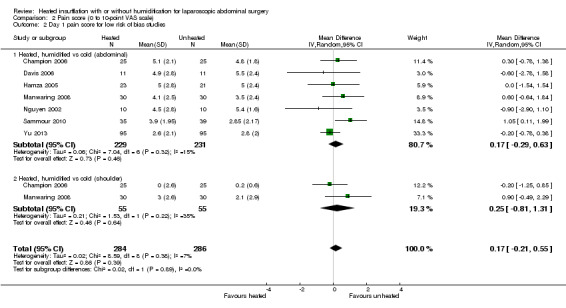
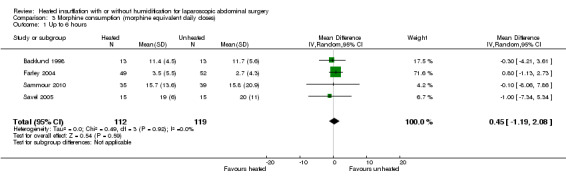
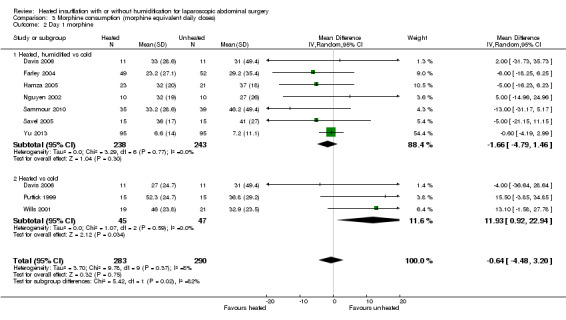
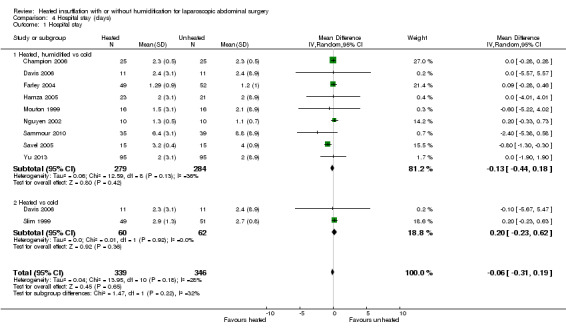
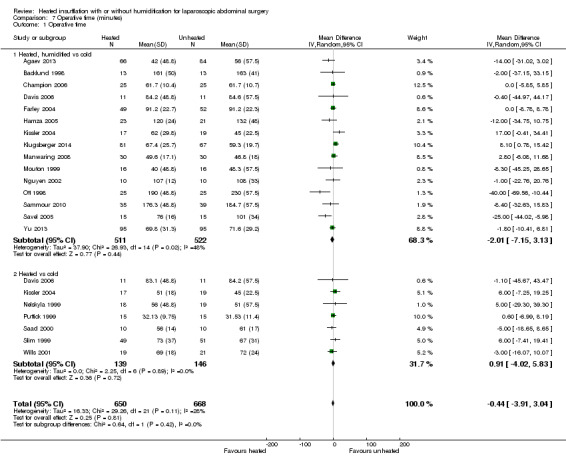
Main results: We included 22 studies in this updated analysis, including six new trials with 584 additional participants, resulting in a total of 1428 participants. The risk of bias was low in 11 studies, high in one study and unclear in the remaining studies, due primarily to failure to report methodology for randomisation, and allocation concealment or blinding, or both. Fourteen studies examined intraoperative core temperatures among heated and humidified insufflation cohorts and core temperatures were higher compared to cold gas insufflation (MD 0.31 °C, 95% CI, 0.09 to 0.53, I2 = 88%, P = 0.005) (low-quality evidence). If the analysis was limited to the eight studies at low risk of bias, this result became non-significant but remained heterogeneous (MD 0.18 °C, 95% CI, -0.04 to 0.39, I2= 81%, P = 0.10) (moderate-quality evidence).In comparison to the cold CO2 group, the meta-analysis of the heated, non-humidified group also showed no statistically significant difference between groups. Core temperature was statistically, significantly higher in the heated, humidified CO2 with external warming groups (MD 0.29 °C, 95% CI, 0.05 to 0.52, I2 = 84%, P = 0.02) (moderate-quality evidence). Despite the small difference in temperature of 0.31 °C with heated CO2, this is unlikely to be of clinical significance.For postoperative pain scores, there were no statistically significant differences between heated and cold CO2, either overall, or for any of the subgroups assessed. Interestingly, morphine-equivalent use was homogeneous and higher in heated, non-humidified insufflation compared to cold insufflation for postoperative day one (MD 11.93 mg, 95% CI 0.92 to 22.94, I2 = 0%, P = 0.03) (low-quality evidence) and day two (MD 9.79 mg, 95% CI 1.58 to 18.00, I2 = 0%, P = 0.02) (low-quality evidence). However, morphine use was not significantly different six hours postoperatively or in any humidified insufflation groups.There was no apparent effect on length of hospitalisation, lens fogging or length of operation with heated compared to cold gas insufflation, with or without humidification. Recovery room time was shorter in the heated cohort (MD -26.79 minutes, 95% CI -51.34 to -2.25, I2 = 95%, P = 0.03) (low-quality evidence). When the one and only unclear-risk study was removed from the analysis, the difference in recovery-room time became non-significant and the studies were statistically homogeneous (MD -1.22 minutes, 95% CI, -6.62 to 4.17, I2 = 12%, P = 0.66) (moderate-quality evidence).There were also no differences in the frequency of major adverse events that occurred in the cold or heated cohorts.These results should be interpreted with caution due to some limitations. Heterogeneity of core temperature remained significant despite subgroup analysis, likely due to variations in the study design of the individual trials, as the trials had variations in insufflation gas temperatures (35 ºC to 37 ºC), humidity ranges (88% to 100%), gas volumes and location of the temperature probes. Additionally, some of the trials lacked specific study design information making evaluation difficult.
Authors' conclusions: While heated, humidified gas leads to mildly smaller decreases in core body temperatures, clinically this does not account for improved patient outcomes, therefore, there is no clear evidence for the use of heated gas insufflation, with or without humidification, compared to cold gas insufflation in laparoscopic abdominal surgery.
Conflict of interest statement
DWB: no conflict of interestJD: no conflict of interestNS: no conflict of interestNM: no conflict of interestXS: no conflict of interestGH: no conflict of interestSK: no conflict of interest
Figures






















Update of
-
Heated CO(2) with or without humidification for minimally invasive abdominal surgery.Cochrane Database Syst Rev. 2011 Jan 19;(1):CD007821. doi: 10.1002/14651858.CD007821.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2016 Oct 19;10:CD007821. doi: 10.1002/14651858.CD007821.pub3. PMID: 21249696 Updated.
References
References to studies included in this review
Agaev 2013 {published data only}
-
- Agaev BA, Muslimov GF, Ibragimov TR, Alieva GR. The efficacy of the moisture and warmed CO(2) for laparoscopic surgery. Khirurgiia (Mosk) 2013;11:35‐9. - PubMed
Backlund 1998 {published data only}
-
- Backlund M, Kellokumpu I, Scheinin T, Smitten K, Tikkanen I, Lindgren L. Effect of temperature of insufflated CO2 during and after prolonged laparoscopic surgery. Surgical Endoscopy 1998;12(9):1126‐30. - PubMed
Champion 2006 {published data only}
-
- Champion JK, Williams M. Prospective randomized trial of heated humidified versus cold dry carbon dioxide insufflation during laparoscopic gastric bypass. Surgery for Obesity and Related Diseases 2006;2(4):445‐9; discussion 449‐50. - PubMed
Davis 2006 {published data only}
-
- Davis SS, Mikami DJ, Newlin M, Needleman BJ, Barett MS, Fries R, et al. Heating and humidifying of carbon dioxide during pneumoperitoneum is not indicated: a prospective randomized trial. Surgical Endoscopy 2006;20(1):153‐8. - PubMed
Demco 2001 {published data only}
-
- Demco L. Effect of heating and humidifying gas on patients undergoing awake laparoscopy. The Journal of the American Association of Gynecologic Laparoscopists 2001;8(2):247‐51. - PubMed
Farley 2004 {published data only}
-
- Farley DR, Greenlee SM, Larson DR, Harrington JR. Double‐blind, prospective, randomized study of warmed, humidified carbon dioxide insufflation vs standard carbon dioxide for patients undergoing laparoscopic cholecystectomy. Archives of Surgery (Chicago, Ill: 1960) 2004;139(7):739‐4. - PubMed
Hamza 2005 {published data only}
-
- Hamza MA, Schneider BE, White PF, Recart A, Villegas L, Ogunnaike B, et al. Heated and humidified insufflation during laparoscopic gastric bypass surgery: effect on temperature, postoperative pain, and recovery outcomes. Journal of Laparoendoscopic & Advanced Surgical Techniques. Part A 2005;15(1):6‐12. - PubMed
Kissler 2004 {published data only}
-
- Kissler S, Haas M, Strohmeier R, Schmitt H, Rody A, Kaufmann M, et al. Effect of humidified and heated CO2 during gynecologic laparoscopic surgery on analgesic requirements and postoperative pain. The Journal of the American Association of Gynecologic Laparoscopists 2004;11(4):473‐7. - PubMed
Klugsberger 2014 {published data only}
-
- Klugsberger B, Schreiner M, Rothe A, Haas D, Oppelt P, Shamiyeh A. Warmed, humidified carbon dioxide insufflation versus standard carbon dioxide in laparoscopic cholecystectomy: a double‐blinded randomized controlled trial. Surgical Endoscopy 2014;28.9:2656‐60. - PubMed
Lee 2011 {published data only}
Manwaring 2008 {published data only}
-
- Manwaring JM, Readman E, Maher PJ. The effect of heated humidified carbon dioxide on postoperative pain, core temperature, and recovery times in patients having laparoscopic surgery: A randomized controlled trial. Journal of Minimally Invasive Gynecology 2008;15(2):161‐5. [DOI: 10.1016/j.jmig.2007.09.007] - DOI - PubMed
Mouton 1999 {published data only}
-
- Mouton WG, Bessell JR, Millard SH, Baxter PS, Maddern GJ. A randomized controlled trial assessing the benefit of humidified insufflation gas during laparoscopic surgery. Surgical Endoscopy 1999;13(2):106‐8. - PubMed
Nelskyla 1999 {published data only}
-
- Nelskyla K, Yli‐Hankala A, Sjoberg J, Korhonen I, Korttila K. Warming of insufflation gas during laparoscopic hysterectomy: effect on body temperature and the autonomic nervous system. Acta Anaesthesiological Scandinavica 1999;43(10):974‐8. - PubMed
Nguyen 2002 {published data only}
-
- Nguyen NT, Furdui G, Fleming NW, Lee SJ, Goldman CD, Singh A, et al. Effect of heated and humidified carbon dioxide gas on core temperature and postoperative pain: a randomized trial. Surgical Endoscopy 2002;16(7):1050‐4. - PubMed
Ott 1998 {published data only}
-
- Ott DE, Reich H, Love B, McCorvey R, Toledo A, Liu CY, et al. Reduction of laparoscopic‐induced hypothermia, postoperative pain and recovery room length of stay by pre‐conditioning gas with the Insuflow device: a prospective randomized controlled multi‐center study. Journal of the Society of Laparoendoscopic Surgeons 1998;2(4):321‐9. - PMC - PubMed
Puttick 1999 {published data only}
-
- Puttick MI, Scott‐Coombes DM, Dye J, Nduka CC, Menzies‐Gow NM, Mansfield AO, et al. Comparison of immunologic and physiologic effects of CO2 pneumoperitoneum at room and body temperatures. Surgical Endoscopy 1999;13(6):572‐5. - PubMed
Saad 2000 {published data only}
-
- Saad S, Minor I, Mohri T, Nagelschmidt M. The clinical impact of warmed insufflation carbon dioxide gas for laparoscopic cholecystectomy. Surgical Endoscopy 2000;14(9):787‐90. - PubMed
Sammour 2010 {published data only}
Savel 2005 {published data only}
-
- Savel RH, Balasubramanya S, Lasheen S, Gaprindashvili T, Arabov E, Fazylov RM, et al. Beneficial effects of humidified, warmed carbon dioxide insufflation during laparoscopic bariatric surgery: a randomized clinical trial. Obesity Surgery 2005;15(1):64‐9. - PubMed
Slim 1999 {published data only}
-
- Slim K, Bousquet J, Kwiatkowski F, Lescure G, Pezet D, Chipponi J. Effect of CO(2) gas warming on pain after laparoscopic surgery: a randomized double‐blind controlled trial. Surgical Endoscopy 1999;13(11):1110‐4. - PubMed
Wills 2001 {published data only}
-
- Wills VL, Hunt DR, Armstrong A. A randomized controlled trial assessing the effect of heated carbon dioxide for insufflation on pain and recovery after laparoscopic fundoplication. Surgical Endoscopy 2001;15(2):166‐70. - PubMed
Yu 2013 {published data only}
-
- Yu TC, Hamill JK, Liley A, Hill AG. Warm, humidified carbon dioxide gas insufflation for laparoscopic appendicectomy in children: a double‐blinded randomized controlled trial. Annals of Surgery 2013;257(1):44‐53. - PubMed
References to studies excluded from this review
Barragan 2005 {published data only}
-
- Barragan AB, Frezza EE. Impact of a warm gas insufflation on operating‐room ergonometrics during laparoscopic gastric bypass: a pilot study. Obesity Surgery 2005;15(1):70‐2. - PubMed
Benavides 2009 {published data only}
Beste 2006 {published data only}
-
- Beste TM, Daucher JA, Holbert D. Humidified compared with dry, heated carbon dioxide at laparoscopy to reduce pain. Obstetrics and Gynecology 2006;107(2 pt 1):263‐8. - PubMed
Herrmann 2015 {published data only}
Monagle 1993 {published data only}
-
- Monagle J, Bradfield S, Nottle P. Carbon dioxide, temperature and laparoscopic cholecystectomy. The Australian and New Zealand Journal of Surgery 1993;63(3):186‐9. - PubMed
Mouton 2001 {published data only}
-
- Mouton WG, Naef M, Bessell JR, Otten KT, Wagner HE, Maddern GJ. A randomized controlled trial to determine the effect of humidified carbon dioxide (CO2) insufflation on postoperative pain following thoracoscopic procedures. Surgical Endoscopy 2001;15(6):579‐81. - PubMed
Ott 1991 {published data only}
-
- Ott DE. Correction of laparoscopic insufflation hypothermia. Journal of Laparoendoscopic Surgery 1991;1(4):183‐6. - PubMed
Pu 2014 {published data only}
-
- Pu Y, Cen G, Sun J, Gong J, Zhang Y, Zhang M, et al. Warming with an underbody warming system reduces intraoperative hypothermia in patients undergoing laparoscopic gastrointestinal surgery: a randomized controlled study. International Journal of Nursing Studies 2014;51(2):181‐9. - PubMed
Siebzehnrubl 2001 {published data only}
-
- Siebzehnruebl E, Haas M, Schmidt H, Lang N. Warm and humidified CO2 does not improve the postoperative pain score after laparoscopy‐a prospective, randomized and double blinded study. Human Reproduction June 2001;Abstracts of the 17th Annual Meeting of the ESHRE:216‐7.
Tohme 2010 {published data only}
-
- Tohme S, Shantha Kumara M, Yan CX, Nasar A, Cekic V, Whelan R. Effect of warmed, humidified CO2 gas on cytokine response to minimally invasive colorectal surgery: a randomized trial. Diseases of the Colon & Rectum 2010;53:4.
Trevelyan 2011 {published data only}
-
- Trevelyan S, Mason C, Chan A, Baird D, Flook D. Does humidified warmed CO2 insufflation gas improve post‐operative pain control in laparoscopic cholecystectomy? A randomized controlled trial. British Journal of Surgery 2011;98(s3):1‐79.
Yeh 2007 {published data only}
-
- Yeh CH, Kwok SY, Chan MK, Tjandra JJ. Prospective, case‐matched study of heated and humidified carbon dioxide insufflation in laparoscopic colorectal surgery. Colorectal Disease 2007;9(8):695‐700. - PubMed
References to studies awaiting assessment
Sutton 2016 {published data only}
-
- Sutton E, Bellini G, Kumara HS, Yan X, Njoh L, Cekic V, et al. Warm and humidified vs cold and dry CO2 pneumoperitoneum in minimally invasive colon resection: a randomized controlled trial. Surgical Endoscopy 2016;30(S1):317. - PubMed
Additional references
Beilin 1998
-
- Beilin B, Shavit Y, Razumovsky J, Wolloch Y, Zeidel A, Bessler H. Effects of mild perioperative hypothermia on cellular immune responses. Anesthesiology 1998;89(5):1133‐40. [9822001] - PubMed
Cork 1983
-
- Cork RC, Vaughan RW, Humphrey LS. Precision and accuracy of intraoperative temperature monitoring . Anesthesia & Analgesia 1983;62:211‐4. - PubMed
Dindo 2004
Egger 1997
Frank 1993
-
- Frank SM, Beattie C, Christopherson R, Norris EJ, Perler BA, Williams GM, et al. Unintentional hypothermia is associated with postoperative myocardial ischemia. The Perioperative Ischemia Randomized Anesthesia Trial Study Group. Anesthesiology 1993;78(3):468‐76. [8457047] - PubMed
Frank 1997
-
- Frank SM, Fleisher LA, Breslow MJ, Higgins MS, Olson KF, Kelly S, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA 1997;277(14):1127‐34. [PUBMED: 9087467] - PubMed
Higgins 2003
Higgins 2011
-
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Janson 2004
Macario 2002
-
- Macario A. What are the most important risk factors for a patient's developing intraoperative hypothermia?. Anesthesia and Analgesia 2002;94(1):215‐20. [11772832] - PubMed
Moher 2009
Neudecker 2002
-
- Neudecker J, Sauerland S, Neugebauer E, Bergamaschi R, Bonjer HJ, Cuschieri A, et al. The European Association for Endoscopic Surgery clinical practice guideline on the pneumoperitoneum for laparoscopic surgery. Surgical Endoscopy 2002;16(7):1121‐43. [PUBMED: 12015619] - PubMed
Putzu 2007
-
- Putzu M, Casati A, Berti M, Pagliarini G, Fanelli G. Clinical complications, monitoring and management of perioperative mild hypothermia: anesthesiological features. Acta Bio‐Medica de l Ateneo Parmense 2007;78(3):163‐9. [PUBMED: 18330074] - PubMed
Qadan 2009
Rajagopalan 2008
-
- Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology 2008;108(1):71‐7. - PubMed
RevMan 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sajid 2008
-
- Sajid MS, Mallick AS, Rimpel J, Bokari SA, Cheek E, Baig MK. Effect of heated and humidified carbon dioxide on patients after laparoscopic procedures: a meta‐analysis. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 2008;18(6):539‐46. [DOI: 10.1097/SLE.0b013e3181886ff4; 00129689‐200812000‐00001; Sajid:2008p530; PUBMED: 19098656] - DOI - PubMed
Sammour 2008
Schünemann 2009
-
- Schünemann H, Brozek J, Oxman A, editors. The GRADE Working Group 2009. GRADE handbook for grading quality of evidence and strength of recommendation. Available from http://www.cc‐ims/gradepro [updated March 2009]; Vol. version 3.2.
Winkler 2000
-
- Winkler M, Akca O, Birkenberg B, Hetz H, Scheck T, Arkiliç CF, et al. Aggressive warming reduces blood loss during hip arthroplasty. Anesthesia and Analgesia 2000;91:978‐84. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous