

Molecular autopsy in victims of inherited arrhythmias
- PMID: 27761159
- PMCID: PMC5063264
- DOI: 10.1016/j.joa.2015.09.010
Molecular autopsy in victims of inherited arrhythmias
Abstract
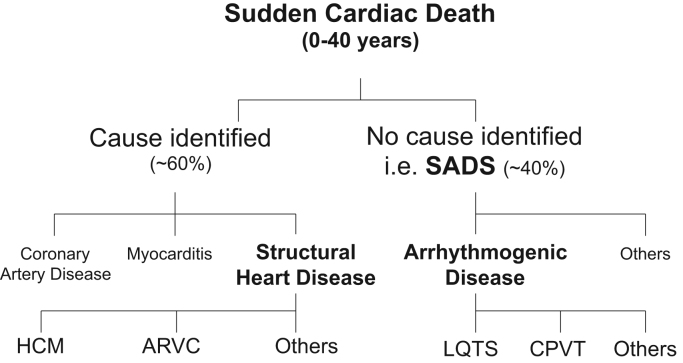
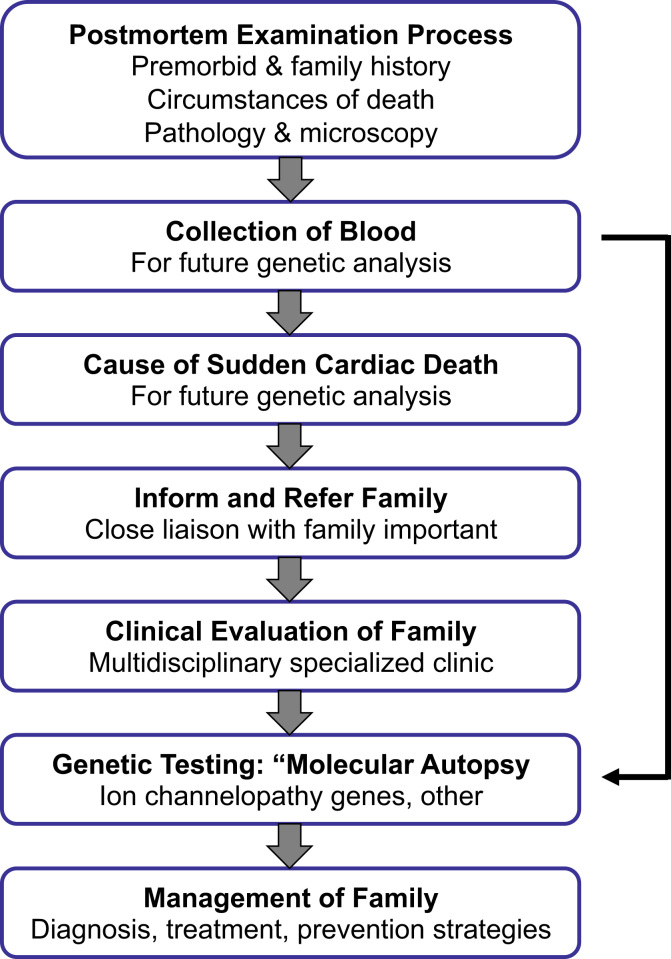
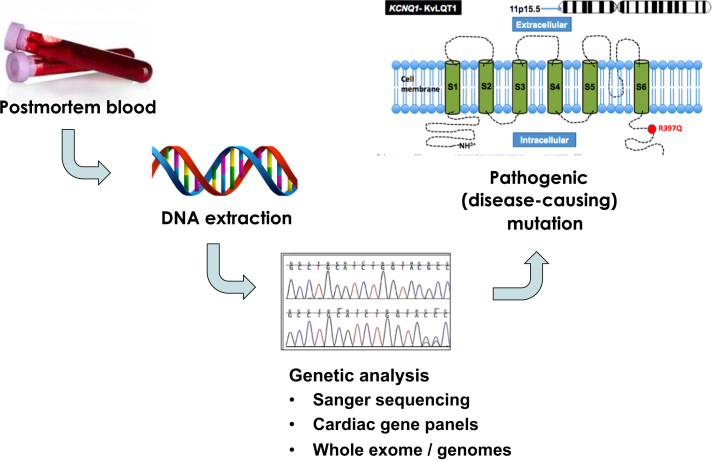
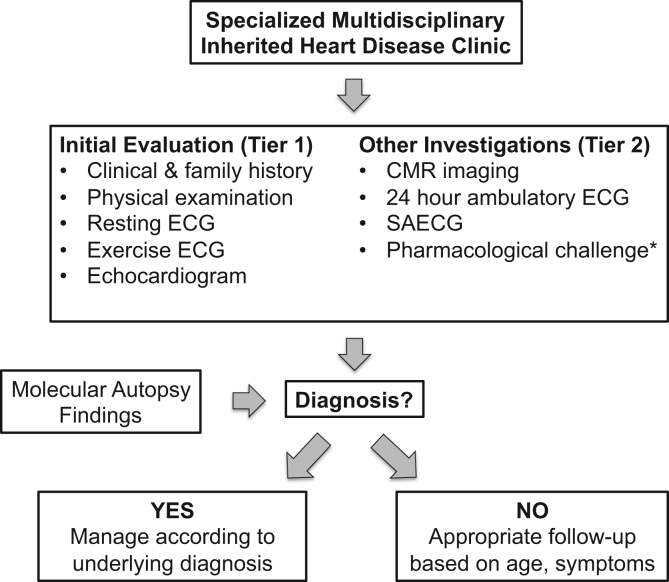
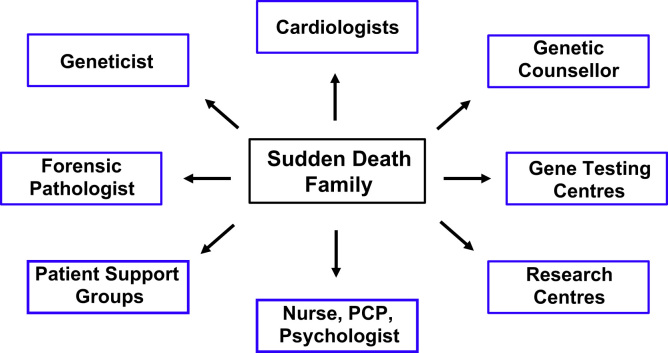
Sudden cardiac death (SCD) is a rare but devastating complication of a number of underlying cardiovascular diseases. While coronary artery disease and acute myocardial infarction are the most common causes of SCD in older populations, inherited cardiac disorders comprise a substantial proportion of SCD cases aged less than 40 years. Inherited cardiac disorders include primary inherited arrhythmogenic disorders such as familial long QT syndrome (LQTS), Brugada syndrome (BrS), catecholaminergic polymorphic ventricular tachycardia (CPVT), and inherited cardiomyopathies, most commonly hypertrophic cardiomyopathy (HCM). In up to 40% of young SCD victims (defined as 1-40 years old, excluding sudden unexplained death in infancy from 0 to 1 years, referred to as SIDS), no cause of death is identified at postmortem [so-called "autopsy negative" or "sudden arrhythmic death syndrome" (SADS)]. Management of families following a SCD includes the identification of the cause of death, based either on premorbid clinical details or the pathological findings at the postmortem. When no cause of death is identified, genetic testing of DNA extracted from postmortem tissue (the molecular autopsy) may identify a cause of death in up to 30% of SADS cases. Targeted clinical testing in a specialized multidisciplinary clinic in surviving family members combined with the results from genetic testing, provide the optimal setting for the identification of relatives who may be at risk of having the same inherited heart disease and are therefore also predisposed to an increased risk of SCD.
Keywords: Genetics; Molecular autopsy; Postmortem; Specialized multidisciplinary clinic; Sudden cardiac death.
Figures
References
-
- Zipes D.P., Wellens H.J. Sudden cardiac death. Circulation. 1998;98:2334–2351. - PubMed
-
- Liberthson R.R. Sudden death from cardiac causes in children and young adults. N Engl J Med. 1996;334:1039–1044. - PubMed
-
- Semsarian C., Sweeting J., Ackerman M.J. Sudden cardiac death in athletes. Br Med J. 2015;350:h1218. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
