

Genetics of Brugada syndrome
- PMID: 27761167
- PMCID: PMC5063259
- DOI: 10.1016/j.joa.2016.07.012
Genetics of Brugada syndrome
Abstract
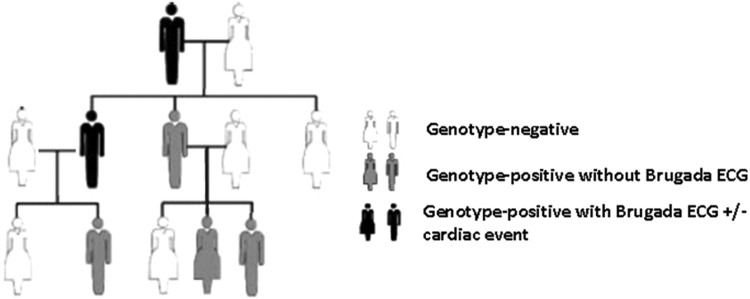
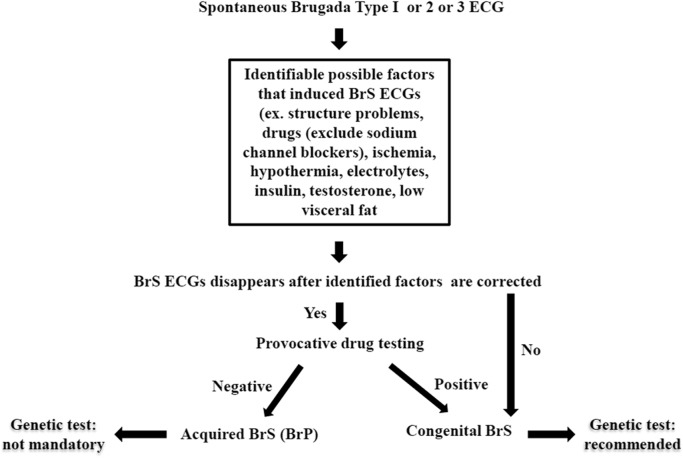
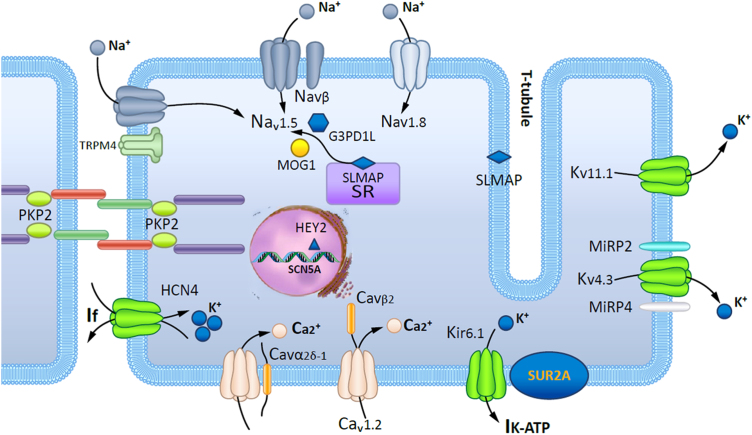
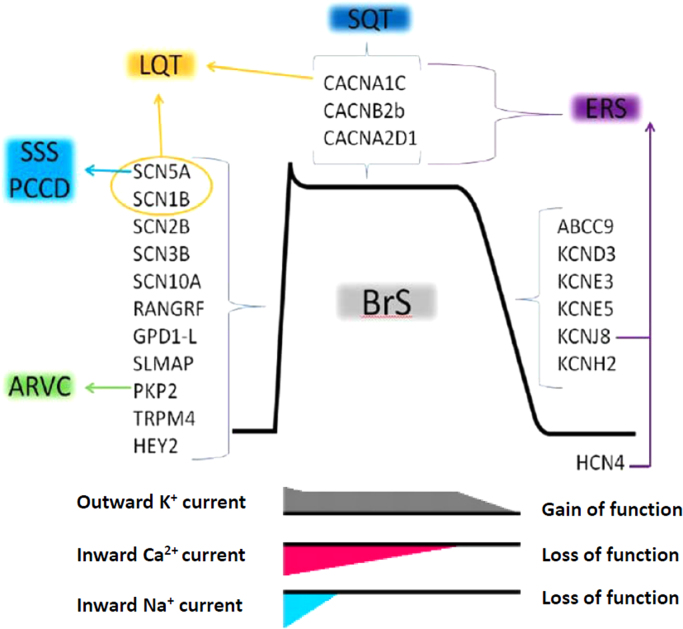
In 1992, the Brugada syndrome (BrS) was recognized as a disease responsible for sudden cardiac death, characterized by a right bundle-branch block with ST segment elevation in the leads V1 and V2. This syndrome is highly associated with sudden cardiac death, especially in young males. BrS is currently diagnosed in patients with ST-segment elevation showing type 1 morphology ≥ 2 mm in ≥1 leads among the right precordial leads V1 or V2 positioned in the 2nd, 3rd, or 4th intercostal space, and occurring either spontaneously or after a provocative drug test by the intravenous administration of Class I antiarrhythmic drugs. With accumulated findings, the BrS inheritance model is believed to be an autosomal dominant inheritable model with incomplete penetrance, although most patients with BrS were sporadic cases. SCN5A, which was identified as the first BrS-associated gene in 1998, has emerged as the most common gene associated with BrS, and more than 10 BrS-associated genes have been identified thereafter. Mutation-specific genetic testing is recommended for the family members and appropriate relatives following the identification of BrS-causative mutations in an index patient. In addition, comprehensive or BrS1 (SCN5A) targeted genetic testing could be useful for patients in whom a cardiologist has established a clinical index of suspicion for BrS based on the patient׳s clinical history, family history, and the expressed electrocardiographic (resting 12-lead ECGs and/or provocative drug challenge testing) phenotype. Over the past 20 years, extensive research in this field has allowed better understanding of the pathophysiology, genetic background, and management of BrS even though controversies still exist. In this review article, a background of genetics, the genetic background of BrS, the genotype and phenotype relationship, the role of genetic screening in clinical practice, and the interpretation of the identified genetic variants have been addressed based on this understanding.
Keywords: Brugada syndrome; Genetics.
Figures
References
-
- Mitchel CR. Biology concept and connections. California; 1997.
-
- Priori S.G., Napolitano C., Gasparini M. Clinical and genetic heterogeneity of right bundle branch block and ST-segment elevation syndrome: a prospective evaluation of 52 families. Circulation. 2000;102(20):2509–2515. - PubMed
-
- Berge K.E., Haugaa K.H., Fruh A. Molecular genetic analysis of long QT syndrome in Norway indicating a high prevalence of heterozygous mutation carriers. Scand J Clin Lab Invest. 2008;68(5):362–368. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
