

Diabetic Macular Edema Pathophysiology: Vasogenic versus Inflammatory
- PMID: 27761468
- PMCID: PMC5059543
- DOI: 10.1155/2016/2156273
Diabetic Macular Edema Pathophysiology: Vasogenic versus Inflammatory
Abstract
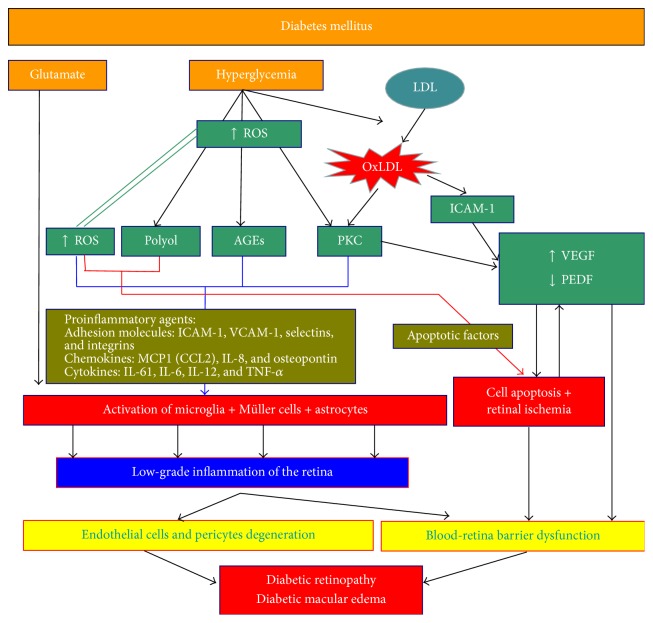
Diabetic macular edema (DME) can cause blindness in diabetic patients suffering from diabetic retinopathy (DR). DM parameters controls (glycemia, arterial tension, and lipids) are the gold standard for preventing DR and DME. Although the vascular endothelial growth factor (VEGF) is known to play a role in the development of DME, the pathological processes leading to the onset of this disease are highly complex and the exact sequence in which they occur is still not completely understood. Angiogenesis and inflammation have been shown to be involved in the pathogenesis of this disease. However, it still remains to be clarified whether angiogenesis following VEGF overexpression is a cause or a consequence of inflammation. This paper provides a review of the data currently available, focusing on VEGF, angiogenesis, and inflammation. Our analysis suggests that angiogenesis and inflammation act interdependently during the development of DME. Knowledge of DME etiology seems to be important in treatments with anti-VEGF or anti-inflammatory drugs. Current diagnostic techniques do not permit us to differentiate between both etiologies. In the future, diagnosing the physiopathology of each patient with DME will help us to select the most effective drug.
Figures
References
-
- International Diabetes Federation. IDF Diabetes Atlas. 6th. Brussels, Belgium: International Diabetes Federation; 2013. http://www.idf.org/diabetesatlas. - PubMed
-
- Romero-Aroca P., De La Riva-Fernandez S., Valls-Mateu A., Sagarra-Alamo R., Moreno-Ribas A., Soler N. Changes observed in diabetic retinopathy: eight-year follow-up of a Spanish population. British Journal of Ophthalmology. 2016;100(10):1366–1371. doi: 10.1136/bjophthalmol-2015-307689. - DOI - PMC - PubMed
-
- Diabetic Retinopathy Guidelines. The Royal College of Ophthalmologists. December 2012, https://www.rcophth.ac.uk/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
