

Review
doi: 10.1007/s40744-016-0046-y.
Epub 2016 Oct 19.
Review of Osteosarcoma and Current Management
Affiliations
- PMID: 27761754
- PMCID: PMC5127970
- DOI: 10.1007/s40744-016-0046-y
Item in Clipboard
Review
Review of Osteosarcoma and Current Management
Rheumatol Ther.
2016 Dec.
Abstract
Osteosarcoma is the most common primary malignancy of bone in children and young adults. This tumor has a very heterogeneous genetic profile and lacks any consistent unifying event that leads to the pathogenesis of osteosarcoma. In this review, some of the important genetic events involved in osteosarcoma will be highlighted. Additionally, the clinical diagnosis of osteosarcoma will be discussed, as well as contemporary chemotherapeutic and surgical management of this tumor. Finally, the review will discuss some of the novel approaches to treating this disease.
Keywords: Limb preservation surgery; Osteosarcoma; Review; Targeted therapy.
Figures
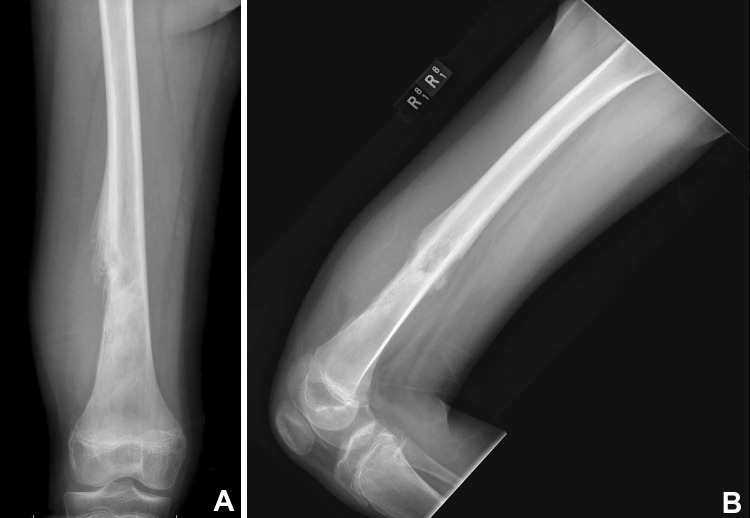
AP (a) and lateral (b) X-rays of an 11-year-old patient with an osteosarcoma of the distal femur. Note the wide zone of transition, discontinuous periosteal reaction, and areas of increased mineralization
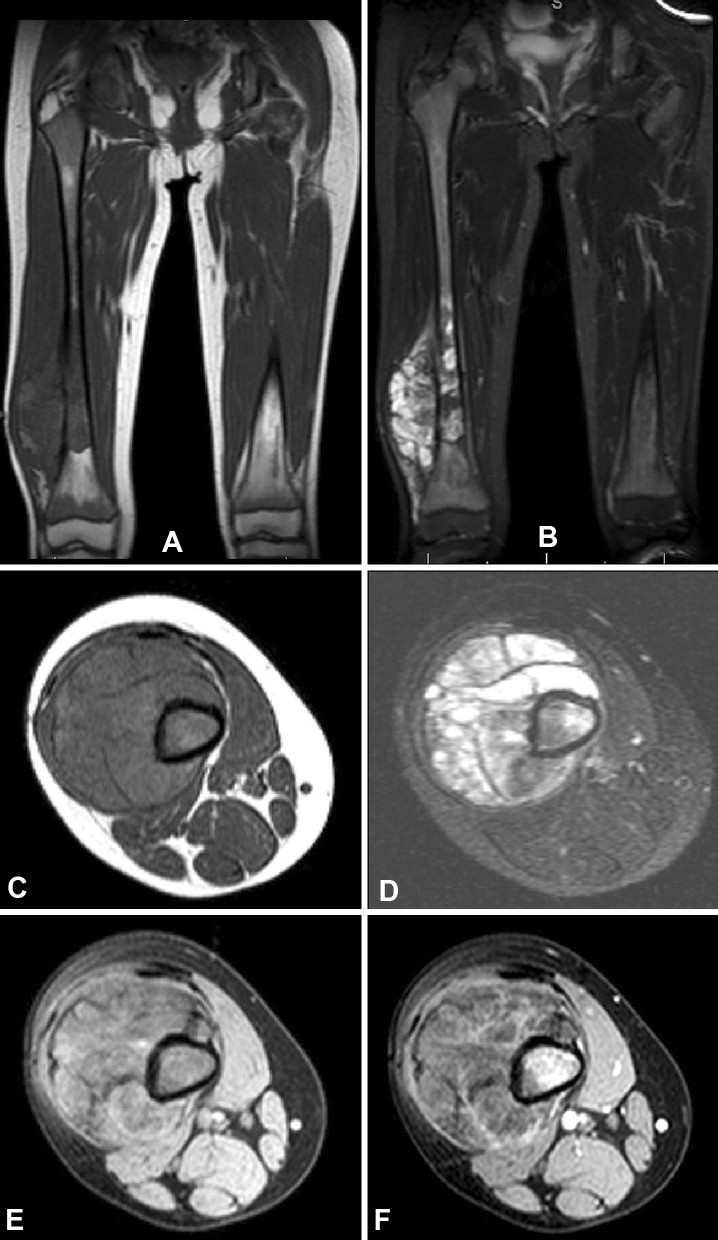
MRI images from the patient in Fig. 1. a Coronal images showing the extent of the marrow abnormality and the soft-tissue mass which appears hypointense on T1 imaging. b STIR imaging illustrating the reaction zone of peritumoral inflammation. c, d Axial images through the tumor reveal a large soft tissue mass with surrounding edema. Pre- (e) and post-contrast (f) axial images show areas of enhancement in the bone and soft tissue, corresponding to sites of increased metabolic activity
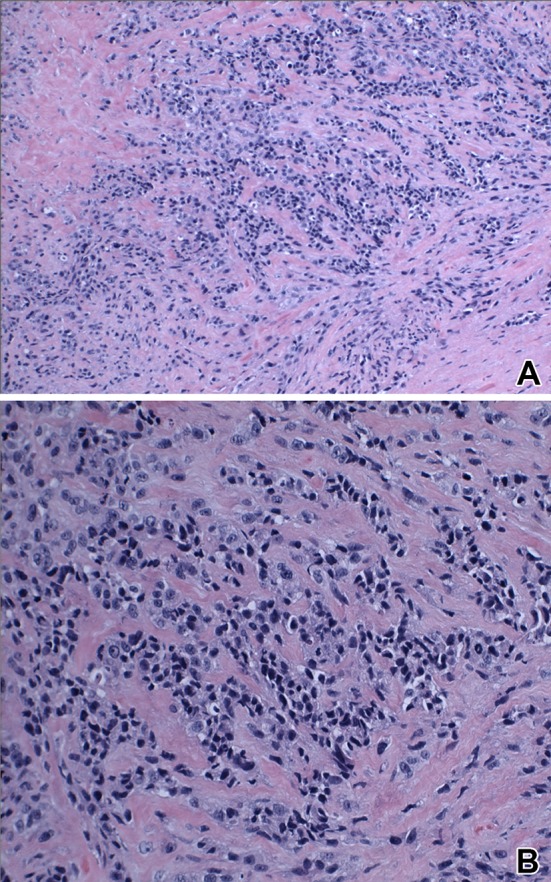
Medium-power (a) and high-power (b) microscopic images of an osteosarcoma specimen, showing high cellularity, nuclear polymorphism, atypia, and disorganized osteoid production

X-ray (a) and MRI (b) of the distal femur of a 13-year-old girl, showing a large solitary lesion. However, staging with bone scan (c) and MRI (d) revealed additional skip metastasis in her ipsilateral femur diaphysis and peritrochanteric area that was not detected with initial imaging. The presence of the skip metastases changed the surgical plan from a distal femur resection to an entire femur resection and reconstruction (e)
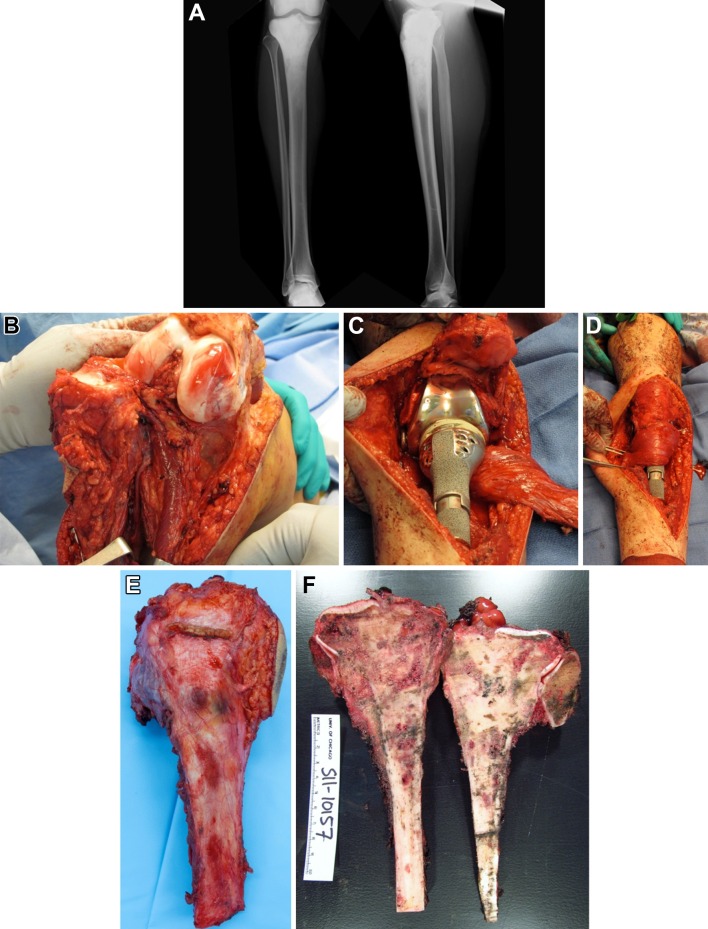
A 22-year-old male with an osteosarcoma of the proximal tibia. XR images (a) show an aggressive lesion of the proximal tibia with abundant osseous matrix. Resection of the tumor mass was performed with care taken to spare the neurovascular bundle (b), and then the defect was reconstructed with a proximal tibia endoprosthesis (c) and a medial gastrocnemius muscle flap for soft-tissue coverage (d). Resected tumor specimen (e, f) and gross pathology examination
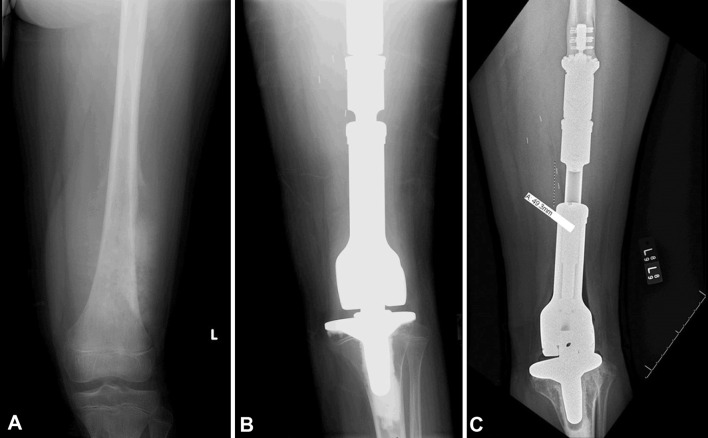
An 11-year-old male patient with a large osteosarcoma of the distal femur that was reconstructed with an expandable endoprosthesis. Preop (a), immediate postop (b), and 2-year postoperative (c) X-ray images are shown. A lengthening of almost 5 cm was achieved with the expandable construct by age 13
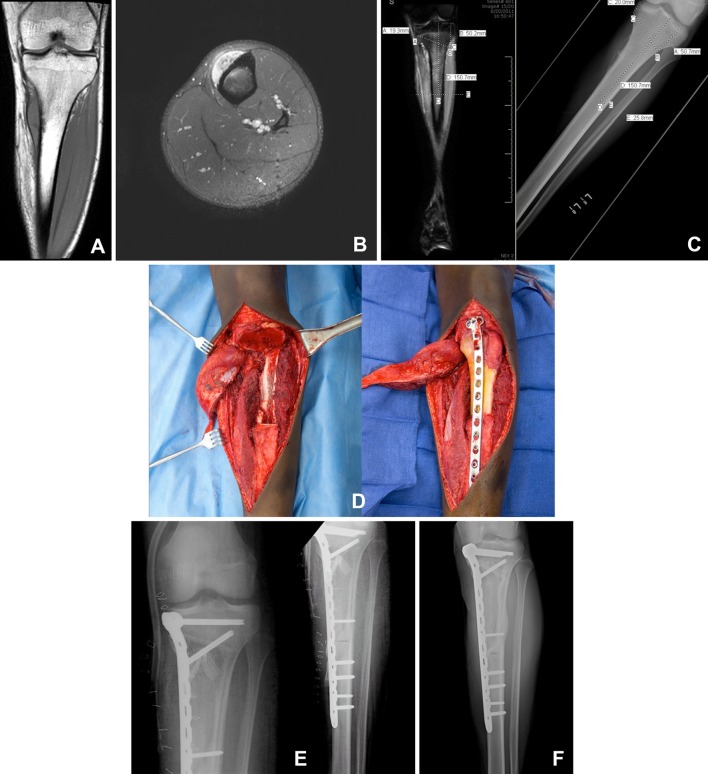
17-year-old male with periosteal osteosarcoma. MRI images (a, b) show the cortically based tumor is located in the metaphysis with some invasion of the marrow and a soft-tissue mass. A polyhedral, metaphysis-sparing bone cut was planned with navigation software (c), and intraoperative guidance was used to assist with the bone cuts according to the preoperative plan (d). A matching allograft was used to fill the defect and fixed to the patient’s remaining bone (e). Two-year follow-up shows robust union at the junction sites (f)
References
-
- Campanacci M. Bone and soft tissue tumors: clinical features, imaging, pathology and treatment. Berlin: Springer; 2013.
-
- Sissons HA. The WHO classification of bone tumors. Recent Res Cancer Res. 1976;54:104–108. - PubMed
-
- Damron TA, Ward WG, Stewart A. Osteosarcoma, chondrosarcoma, and Ewing’s sarcoma: National Cancer Data Base Report. Clin Orthop Relat Res. 2007;459:40–47. - PubMed
-
- Dorfman HD, Czerniak B. Bone cancers. Cancer. 1995;75(1 Suppl):203–210. - PubMed
-
- dos Santos Silva I, Swerdlow AJ. Sex differences in the risks of hormone-dependent cancers. Am J Epidemiol. 1993;138(1):10–28. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
