

Use of Household Cluster Investigations to Identify Factors Associated with Chikungunya Virus Infection and Frequency of Case Reporting in Puerto Rico
- PMID: 27764085
- PMCID: PMC5072658
- DOI: 10.1371/journal.pntd.0005075
Use of Household Cluster Investigations to Identify Factors Associated with Chikungunya Virus Infection and Frequency of Case Reporting in Puerto Rico
Abstract
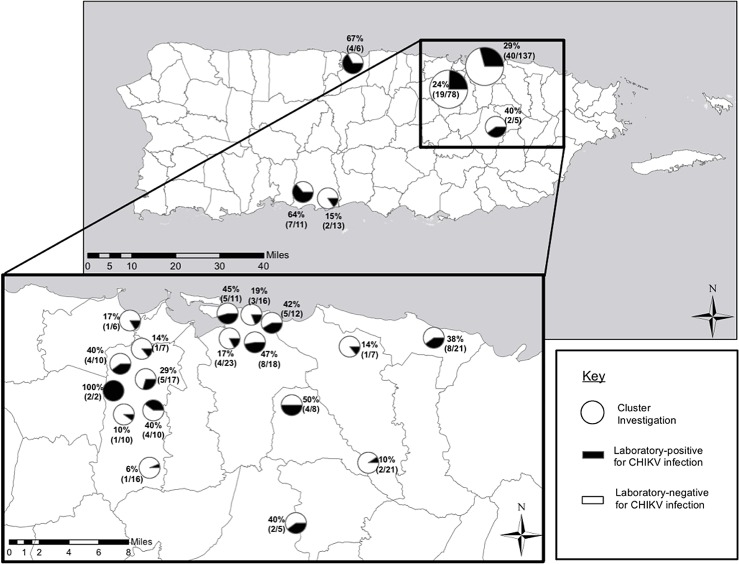
Background: Chikungunya virus (CHIKV) is transmitted by Aedes species mosquitoes and is the cause of an acute febrile illness characterized by potentially debilitating arthralgia. After emerging in the Caribbean in late 2013, the first locally-acquired case reported to public health authorities in Puerto Rico occurred in May 2014. During June-August 2014, household-based cluster investigations were conducted to identify factors associated with infection, development of disease, and case reporting.
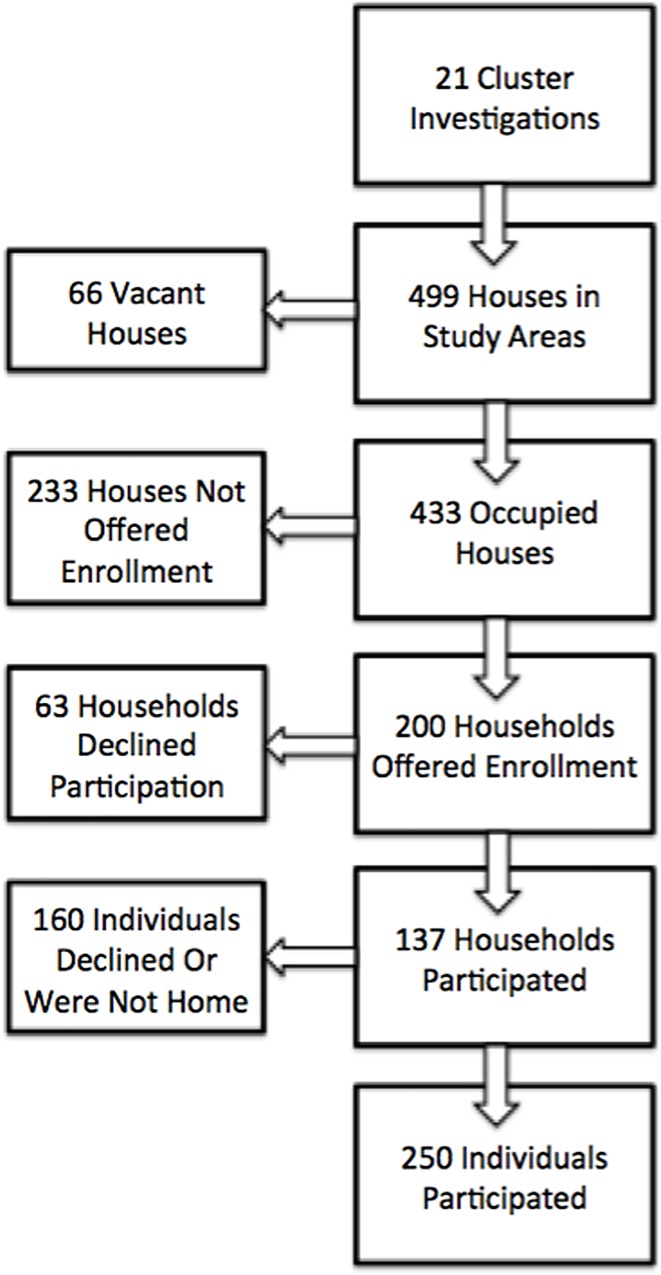
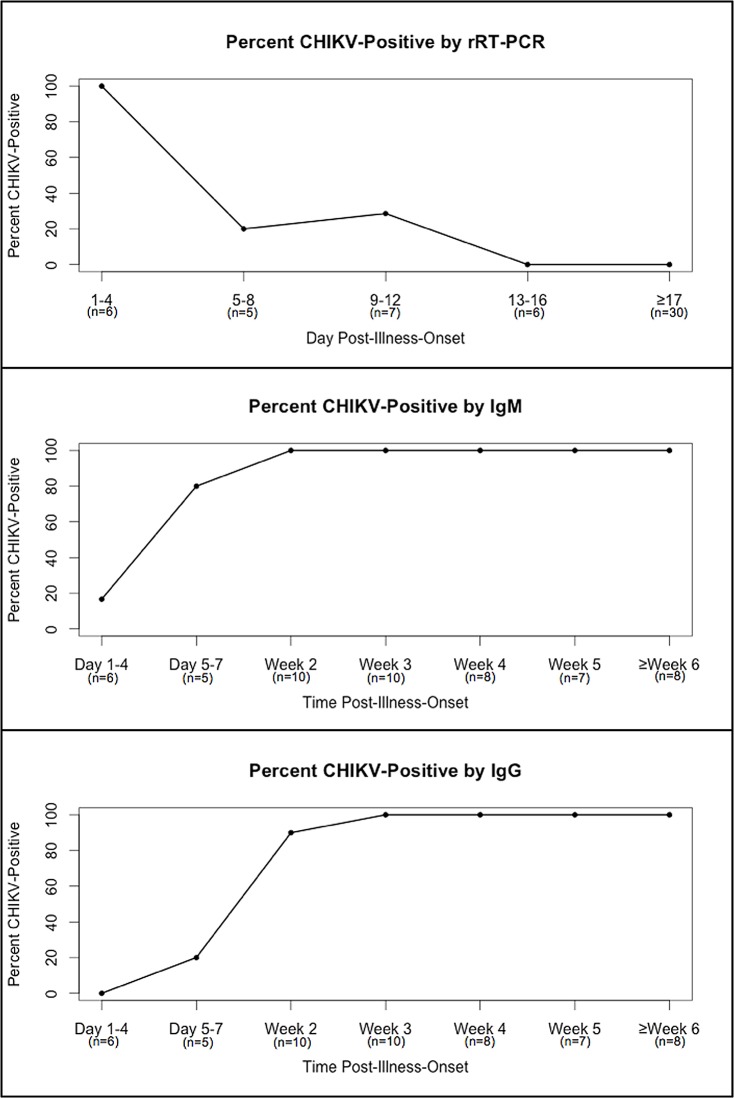
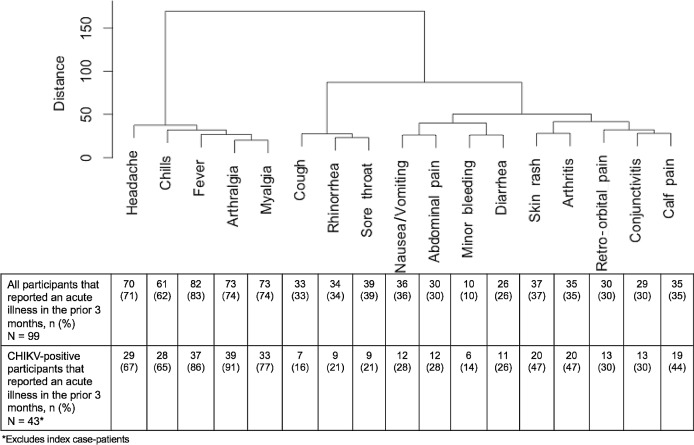
Methodology/principal findings: Residents of households within a 50-meter radius of the residence of laboratory-positive chikungunya cases that had been reported to Puerto Rico Department of Health (PRDH) were offered participation in the investigation. Participants provided a serum specimen and answered a questionnaire that collected information on demographic factors, household characteristics, recent illnesses, healthcare seeking behaviors, and clinical diagnoses. Current CHIKV infection was identified by rRT-PCR, and recent CHIKV infection was defined by detection of either anti-CHIKV IgM or IgG antibody. Among 250 participants, 74 (30%) had evidence of CHIKV infection, including 12 (5%) with current and 62 (25%) with recent CHIKV infection. All specimens from patients with CHIKV infection that were collected within four days, two weeks, and three weeks of illness onset were positive by RT-PCR, IgM ELISA, and IgG ELISA, respectively. Reporting an acute illness in the prior three months was strongly associated with CHIKV infection (adjusted odds ratio [aOR] = 21.6, 95% confidence interval [CI]: 9.24-50.3). Use of air conditioning (aOR = 0.50, 95% CI = 0.3-0.9) and citronella candles (aOR = 0.4, 95% CI = 0.1-0.9) were associated with protection from CHIKV infection. Multivariable analysis indicated that arthralgia (aOR = 51.8, 95% CI = 3.8-700.8) and skin rash (aOR = 14.2, 95% CI = 2.4-84.7) were strongly associated with CHIKV infection. Hierarchical cluster analysis of signs and symptoms reported by CHIKV-infected participants demonstrated that fever, arthralgia, myalgia, headache, and chills tended to occur simultaneously. Rate of symptomatic CHIKV infection (defined by arthralgia with fever or skin rash) was 62.5%. Excluding index case-patients, 22 (63%) participants with symptomatic CHIKV infection sought medical care, of which 5 (23%) were diagnosed with chikungunya and 2 (9%) were reported to PRDH.
Conclusions/significance: This investigation revealed high rates of CHIKV infection among household members and neighbors of chikungunya patients, and that behavioral interventions such as use of air conditioning were associated with prevention of CHIKV infection. Nearly two-thirds of patients with symptomatic CHIKV infection sought medical care, of which less than one-quarter were reportedly diagnosed with chikungunya and one-in-ten were reported to public health authorities. These findings emphasize the need for point-of-care rapid diagnostic tests to optimize identification and reporting of chikungunya patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- CDC, Pan American Health Organization (2012) Preparedness and Response Plan for Chikungunya Virus Introduction in the Caribbean sub-region. Kingston, Jamaica
-
- Gérardin P, Guernier V, Perrau J, Fianu A, Le Roux K, Grivard P, Michault A, de Lamballerie X, Flahault A, Favier F (2008) Estimating Chikungunya prevalence in La Réunion Island outbreak by serosurveys: two methods for two critical times of the epidemic. BMC Infect Dis 8:99 10.1186/1471-2334-8-99 - DOI - PMC - PubMed
-
- Sergon K, Njuguna C, Kalani R, et al. (2008) Seroprevalence of Chikungunya Virus (CHIKV) Infection on Lamu Island, Kenya, October 2004. 78:333–337 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
