

Long-Term Outcomes on Antiretroviral Therapy in a Large Scale-Up Program in Nigeria
- PMID: 27764094
- PMCID: PMC5072640
- DOI: 10.1371/journal.pone.0164030
Long-Term Outcomes on Antiretroviral Therapy in a Large Scale-Up Program in Nigeria
Abstract
Background: While there has been a rapid global scale-up of antiretroviral therapy programs over the past decade, there are limited data on long-term outcomes from large cohorts in resource-constrained settings. Our objective in this evaluation was to measure multiple outcomes during first-line antiretroviral therapy in a large treatment program in Nigeria.
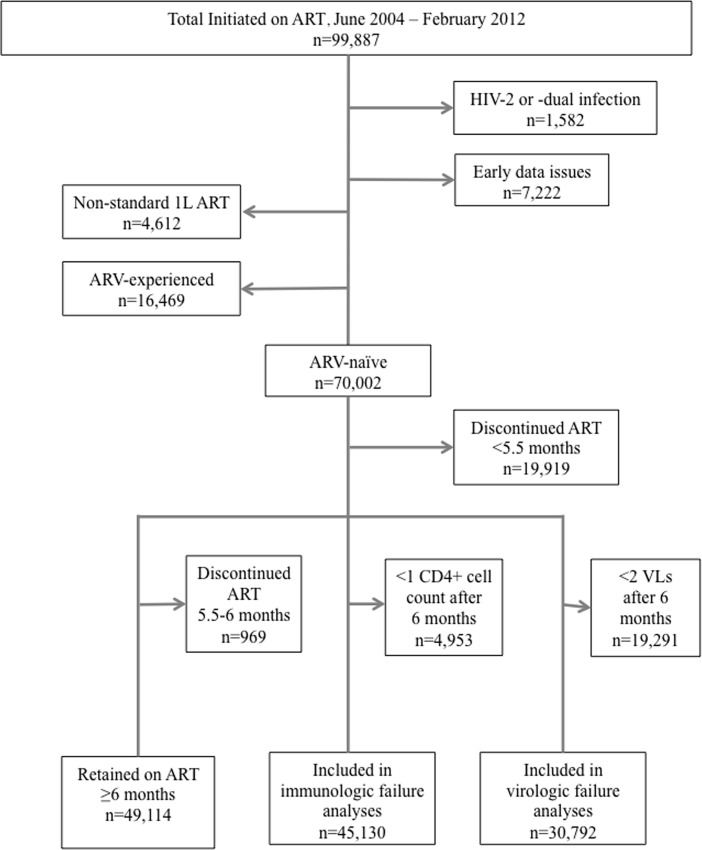
Methods: We conducted a retrospective multi-site program evaluation of adult patients (age ≥15 years) initiating antiretroviral therapy between June 2004 and February 2012 in Nigeria. The baseline characteristics of patients were described and longitudinal analyses using primary endpoints of immunologic recovery, virologic rebound, treatment failure and long-term adherence patterns were conducted.
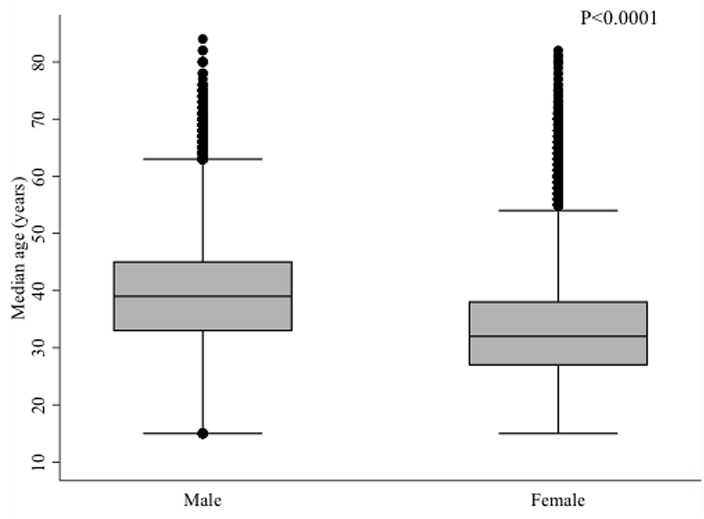
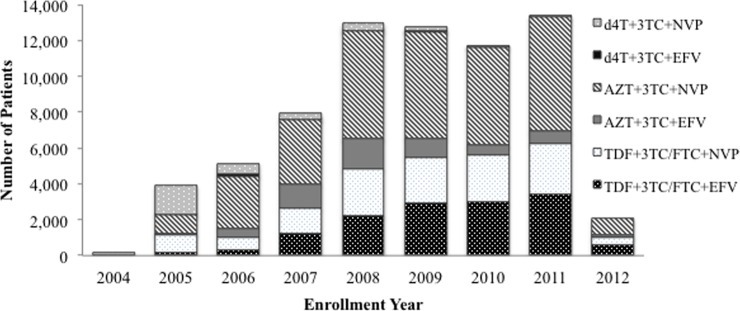
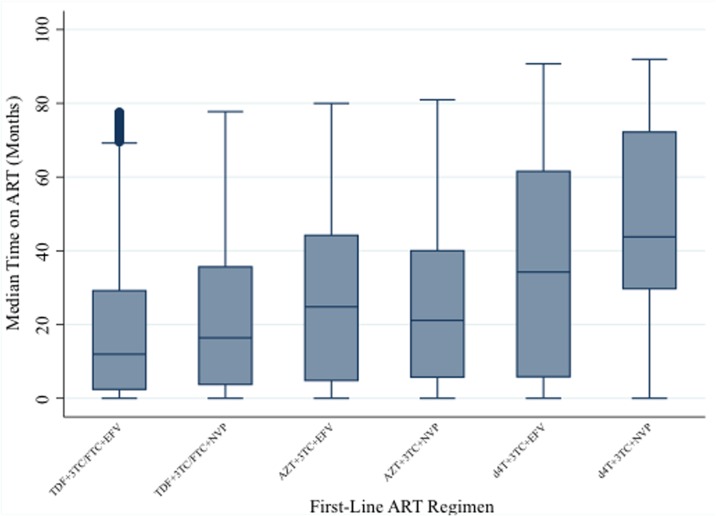
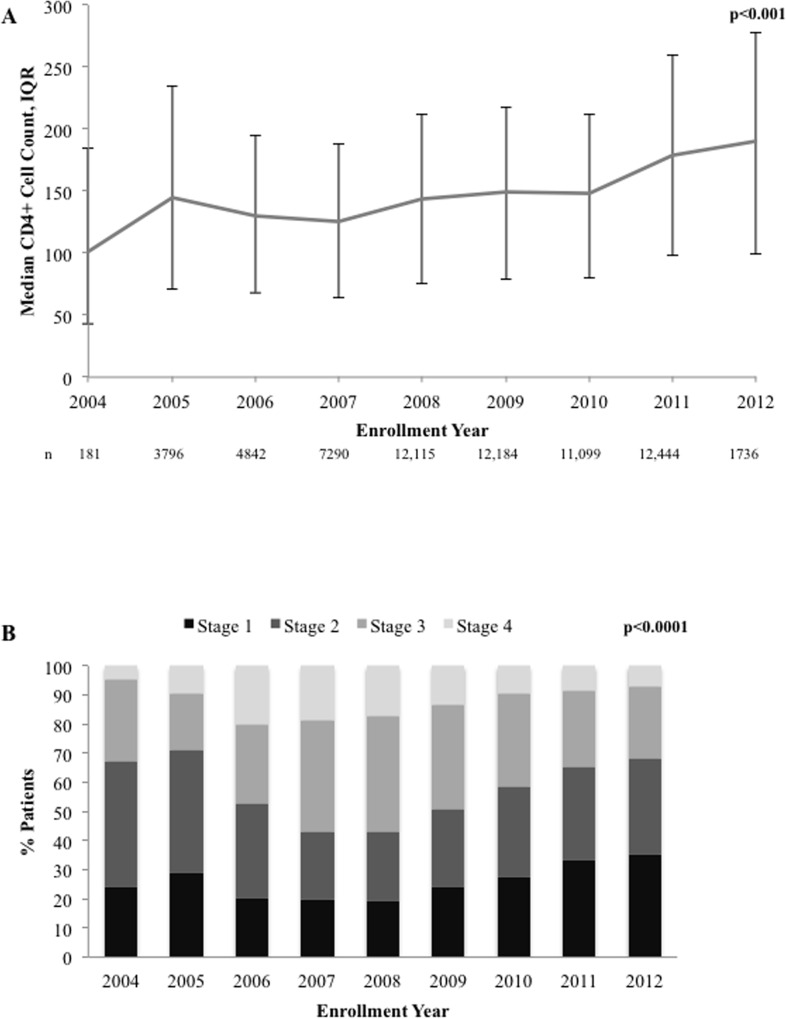
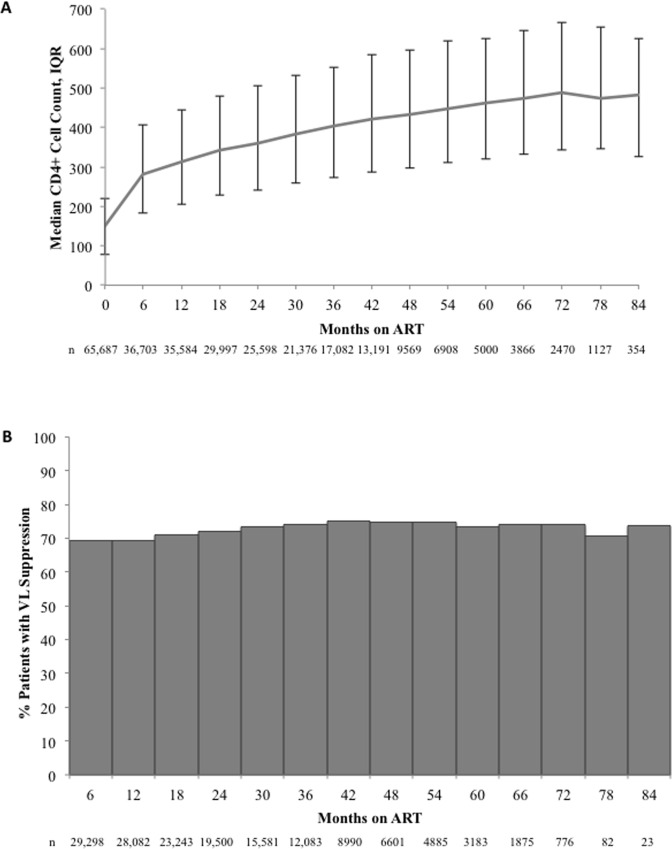
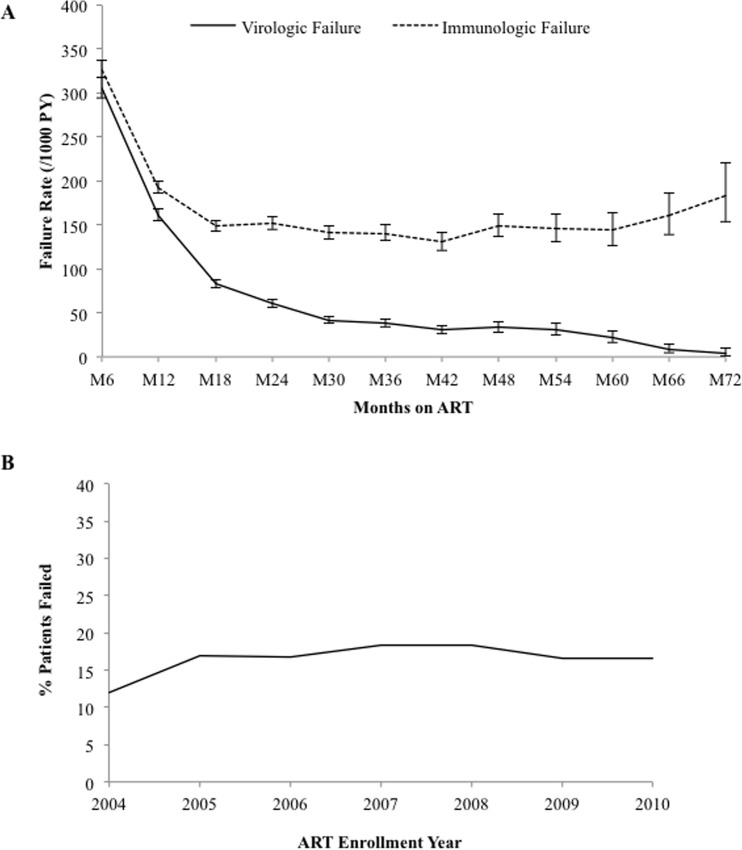
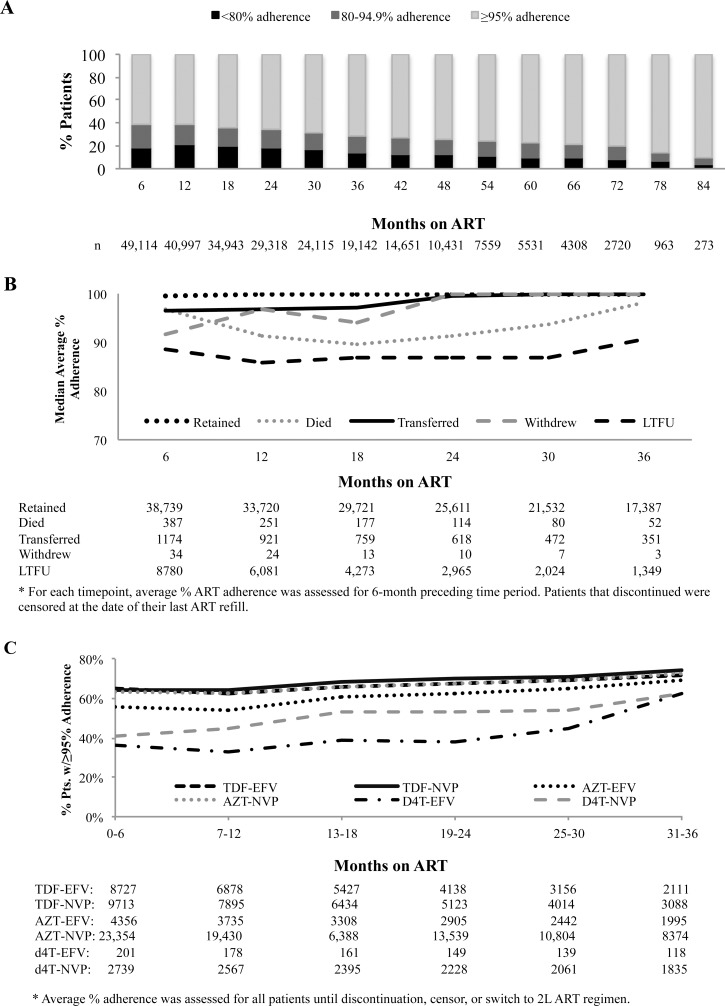
Results: Of 70,002 patients, 65.2% were female and median age was 35 (IQR: 29-41) years; 54.7% were started on a zidovudine-containing and 40% on a tenofovir-containing first-line regimen. Median CD4+ cell counts for the cohort started at 149 cells/mm3 (IQR: 78-220) and increased over duration of ART. Of the 70,002 patients, 1.8% were reported as having died, 30.1% were lost to follow-up, and 0.1% withdrew from treatment. Overall, of those patients retained and with viral load data, 85.4% achieved viral suppression, with 69.3% achieving suppression by month 6. Of 30,792 patients evaluated for virologic failure, 24.4% met criteria for failure and of 45,130 evaluated for immunologic failure, 34.0% met criteria for immunologic failure, with immunologic criteria poorly predicting virologic failure. In adjusted analyses, older age, ART regimen, lower CD4+ cell count, higher viral load, and inadequate adherence were all predictors of virologic failure. Predictors of immunologic failure differed slightly, with age no longer predictive, but female sex as protective; additionally, higher baseline CD4+ cell count was also predictive of failure. Evaluation of long-term adherence patterns revealed that the majority of patients retained through 84 months maintained ≥95% adherence.
Conclusion: While improved access to HIV care and treatment remains a challenge in Nigeria, our study shows that a high quality of care was achieved as evidenced by strong long-term clinical, immunologic and virologic outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- UNAIDS. The Gap Report. 2014. Available: http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/....
-
- Assefa Y, Lynen L, Kloos H, Hill P, Rasschaert F, Hailemariam D, et al. Brief Report: Long-term outcomes and their determinants in patients on antiretroviral treatment in Ethiopia, 2005/6-2011/12: A Retrospective Cohort Study. J Acquir Immune Defic Syndr. 2015; 70: 414–419. 10.1097/QAI.0000000000000753 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
