

Asymmetry Analysis of Macular Inner Retinal Layers for Glaucoma Diagnosis: Swept-Source Optical Coherence Tomography Study
- PMID: 27764166
- PMCID: PMC5072638
- DOI: 10.1371/journal.pone.0164866
Asymmetry Analysis of Macular Inner Retinal Layers for Glaucoma Diagnosis: Swept-Source Optical Coherence Tomography Study
Abstract
Purpose: To report an asymmetry analysis of macular inner retinal layers using swept-source optical coherence tomography (OCT) and to evaluate the utility for glaucoma diagnosis.
Design: Observational, cross-sectional study.
Participants: Seventy normal healthy subjects and 62 glaucoma patients.
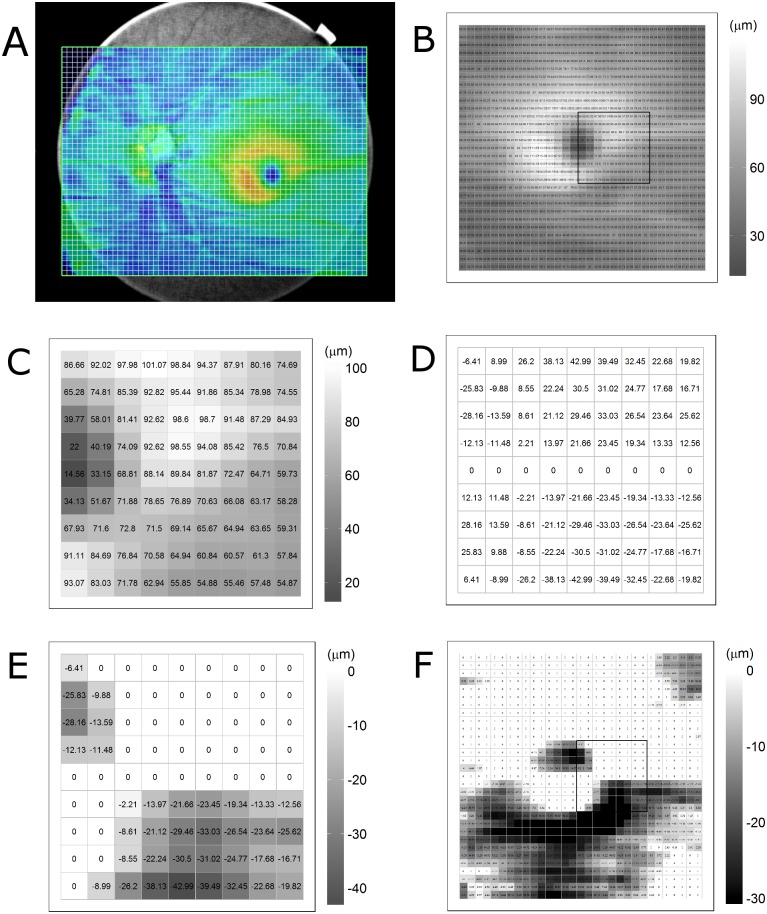
Methods: Three-dimensional scans were acquired from 70 normal subjects and 62 open angle glaucoma patients by swept-source OCT. The thickness of the retinal nerve fiber layer, ganglion cell-inner plexiform layer (GCIPL), ganglion cell complex, and total retina were calculated within a 6.2×6.2 mm macular area divided into a 31×31 grid of 200×200 μm superpixels. For each of the corresponding superpixels, the thickness differences between the subject eyes and contra-lateral eyes and between the upper and lower macula halves of the subject eyes were determined. The negative differences were displayed on a gray-scale asymmetry map. Black superpixels were defined as thickness decreases over the cut-off values.
Results: The negative inter-ocular and inter-hemisphere differences in GCIPL thickness (mean ± standard deviation) were -2.78 ± 0.97 μm and -3.43 ± 0.71 μm in the normal group and -4.26 ± 2.23 μm and -4.88 ± 1.46 μm in the glaucoma group. The overall extent of the four layers' thickness decrease was larger in the glaucoma group than in the normal group (all Ps<0.05). The numbers of black superpixels on all of the asymmetry maps were larger in the glaucoma group than in the normal group (all Ps<0.05). The area under receiver operating characteristic curves of average negative thickness differences in macular inner layers for glaucoma diagnosis ranged from 0.748 to 0.894.
Conclusions: The asymmetry analysis of macular inner retinal layers showed significant differences between the normal and glaucoma groups. The diagnostic performance of the asymmetry analysis was comparable to that of previous methods. These findings suggest that the asymmetry analysis can be a potential ancillary diagnostic tool.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Essock EA, Sinai MJ, Fechtner RD. Interocular symmetry in nerve fiber layer thickness of normal eyes as determined by polarimetry. J Glaucoma. 1999;8:90–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
