

Intensity-modulated radiation therapy achieves better local control compared to three-dimensional conformal radiation therapy for T4-stage nasopharyngeal carcinoma
- PMID: 27764778
- PMCID: PMC5355163
- DOI: 10.18632/oncotarget.12736
Intensity-modulated radiation therapy achieves better local control compared to three-dimensional conformal radiation therapy for T4-stage nasopharyngeal carcinoma
Abstract
Purpose: To examine the survival outcomes and late toxicity profiles of three-dimensional conformal radiation therapy (3DCRT) vs. intensity-modulated radiation therapy (IMRT) for patients with nasopharyngeal carcinoma (NPC).
Methods: Three hundred and seventy-four patients with newly diagnosed, non-metastatic, NPC who were curatively treated with 3DCRT between 2004 and 2006 and 481 patients treated with IMRT between 2007 and 2009 were analyzed. Patients were categorized as having advanced-stage disease (stage III, IVA, and IVB disease; n = 709) or early-stage disease (stage I and II; n = 146). The median follow-up time was 90.3 months for patients treated with 3DCRT and 86.3 months for patients treated with IMRT.
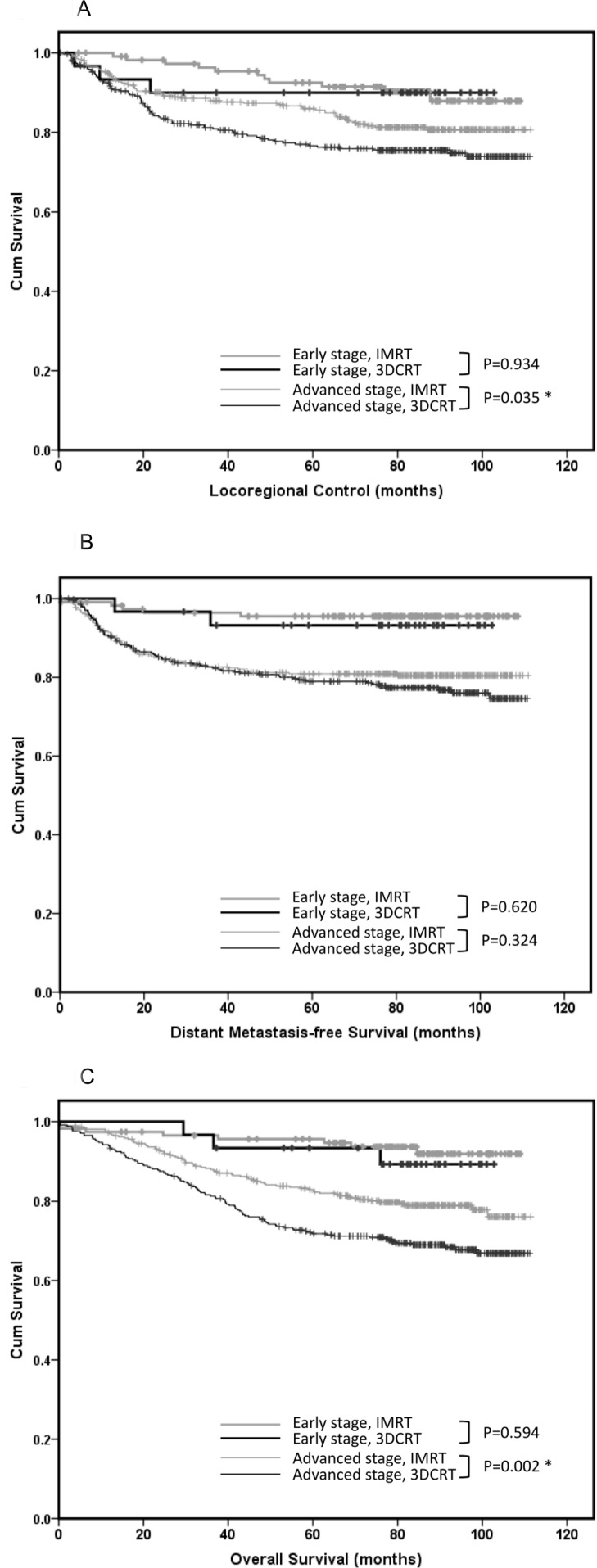
Results: For early-stage patients, the outcomes of IMRT vs. 3DCRT were similar considering locoregional control (LRC), distant metastasis-free survival (DMFS), and overall survival (OS). For advanced-stage patients, IMRT was associated with better LRC compared with 3DCRT (5-year LRC rate: 85.6% vs. 76.6%, respectively; p = 0.035) and OS (5-year OS rate: 82.3% vs. 71.8%, respectively; p = 0.002), whereas DMFS was similar for both treatments (5-year DMFS rate: 80.9% vs. 79.0%, respectively; p = 0.324). Furthermore, the IMRT technique was more beneficial for patients with T4 disease. Late toxicities occurred more frequently in patients treated with 3DCRT than in those treated with IMRT (grade ≥3 neck fibrosis: 6.7% vs. 3.7%, respectively, p = 0.036; radiographic temporal lobe necrosis: 10.2% vs. 4.4%, respectively, p < 0.001).
Conclusions: Compared with 3DCRT, IMRT offered better LRC in patients with advanced-stage non-metastatic NPC, which corresponded with better OS.
Keywords: conformal radiation therapy; intensity-modulated radiation therapy; late toxicities; nasopharyngeal carcinoma; survival outcomes.
Conflict of interest statement
The authors indicate no potential conflicts of interest.
Figures


References
-
- Hong RL, Ting LL, Ko JY, Hsu MM, Sheen TS, Lou PJ, Wang CC, Chung NN, Lui LT. Induction chemotherapy with mitomycin, epirubicin, cisplatin, fluorouracil, and leucovorin followed by radiotherapy in the treatment of locoregionally advanced nasopharyngeal carcinoma. J Clin Oncol. 2001;19:4305–4313. - PubMed
-
- Lee N, Harris J, Garden AS, Straube W, Glisson B, Xia P, Bosch W, Morrison WH, Quivey J, Thorstad W, Jones C, Ang KK. Intensity-modulated radiation therapy with or without chemotherapy for nasopharyngeal carcinoma: radiation therapy oncology group phase II trial 0225. J Clin Oncol. 2009;27:3684–3690. - PMC - PubMed
-
- Kam MK, Chau RM, Suen J, Choi PH, Teo PM. Intensity-modulated radiotherapy in nasopharyngeal carcinoma: dosimetric advantage over conventional plans and feasibility of dose escalation. Int J Radiat Oncol Biol Phys. 2003;56:145–157. - PubMed
-
- Lu SH, Cheng JC, Kuo SH, Lee JJ, Chen LH, Wu JK, Chen YH, Chen WY, Wen SY, Chong FC, Wu CJ, Wang CW. Volumetric modulated arc therapy for nasopharyngeal carcinoma: A dosimetric comparison with TomoTherapy and step-and-shoot IMRT. Radiother Oncol. 2012;104:323–330. - PubMed
-
- Chen JL, Huang YS, Kuo SH, Chen YF, Hong RL, Ko JY, Lou PJ, Tsai CL, Chen WY, Wang CW. Intensity-modulated radiation therapy for T4 nasopharyngeal carcinoma. Treatment results and locoregional recurrence. Strahlenther Onkol. 2013;189:1001–1008. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
