

Prophylactic abdominal drainage for pancreatic surgery
- PMID: 27764898
- PMCID: PMC6611488
- DOI: 10.1002/14651858.CD010583.pub3
Prophylactic abdominal drainage for pancreatic surgery
Update in
-
Prophylactic abdominal drainage for pancreatic surgery.Cochrane Database Syst Rev. 2018 Jun 21;6(6):CD010583. doi: 10.1002/14651858.CD010583.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 Dec 18;12:CD010583. doi: 10.1002/14651858.CD010583.pub5. PMID: 29928755 Free PMC article. Updated.
Abstract
Background: The use of surgical drains has been considered mandatory after pancreatic surgery. The role of prophylactic abdominal drainage to reduce postoperative complications after pancreatic surgery is controversial.
Objectives: To assess the benefits and harms of routine abdominal drainage after pancreatic surgery, compare the effects of different types of surgical drains, and evaluate the optimal time for drain removal.
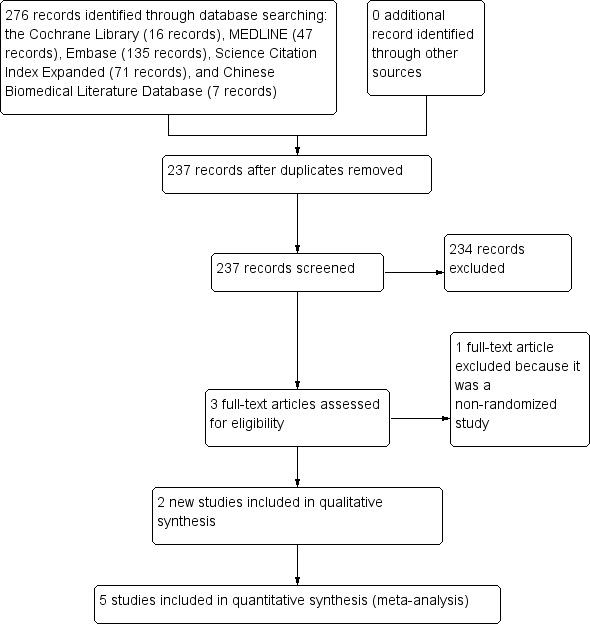
Search methods: For the initial version of this review, we searched the Cochrane Library (2015, Issue 3), MEDLINE (1946 to 9 April 2015), Embase (1980 to 9 April 2015), Science Citation Index Expanded (1900 to 9 April 2015), and Chinese Biomedical Literature Database (CBM) (1978 to 9 April 2015). For this updated review, we searched the Cochrane Library, MEDLINE, Embase, Science Citation Index Expanded, and CBM from 2015 to 28 August 2016.
Selection criteria: We included all randomized controlled trials that compared abdominal drainage versus no drainage in people undergoing pancreatic surgery. We also included randomized controlled trials that compared different types of drains and different schedules for drain removal in people undergoing pancreatic surgery.
Data collection and analysis: We identified five trials (of 985 participants) which met our inclusion criteria. Two review authors independently identified the trials for inclusion, collected the data, and assessed the risk of bias. We performed the meta-analyses using Review Manager 5. We calculated the risk ratio (RR) for dichotomous outcomes and the mean difference (MD) for continuous outcomes with 95% confidence intervals (CI). For all analyses, we employed the random-effects model.
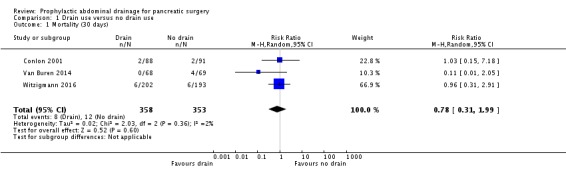
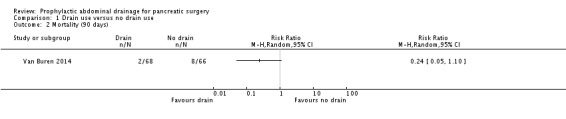
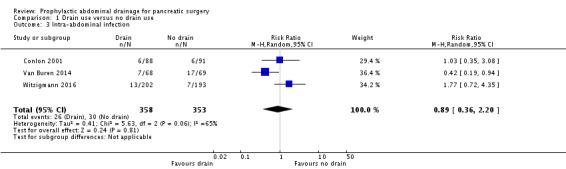
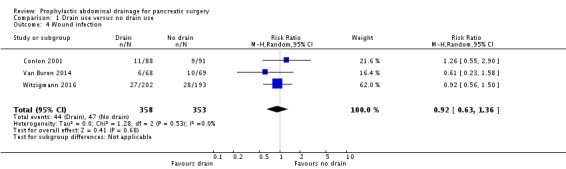
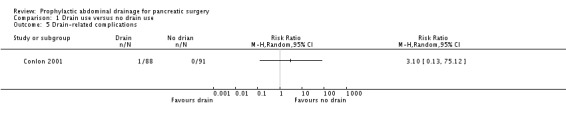
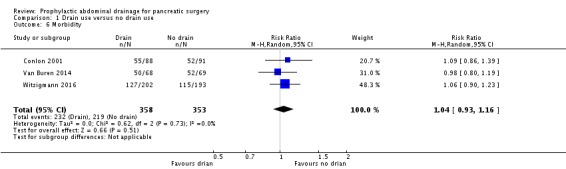
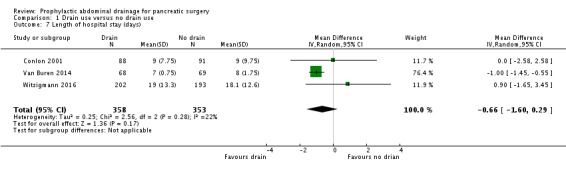
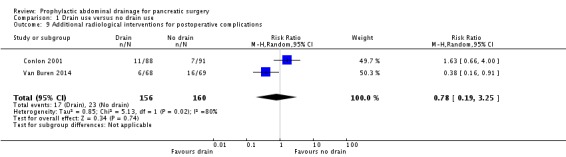
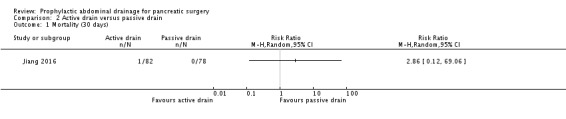
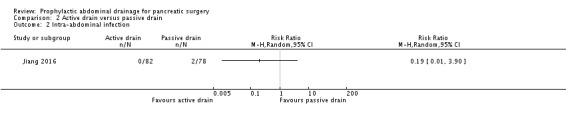
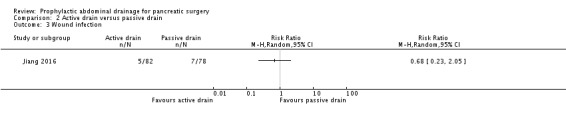
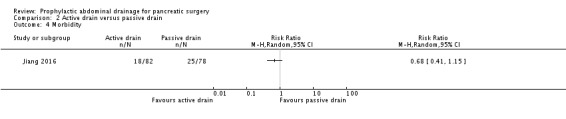
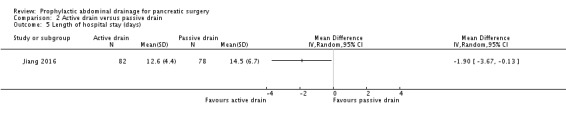
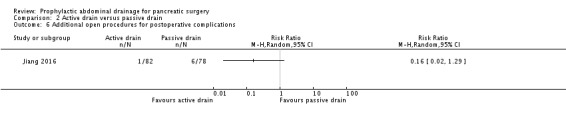
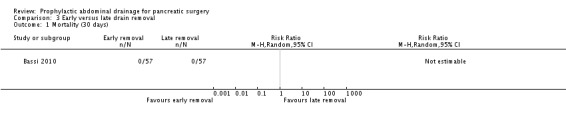
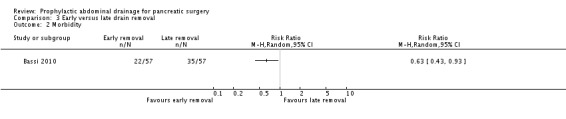
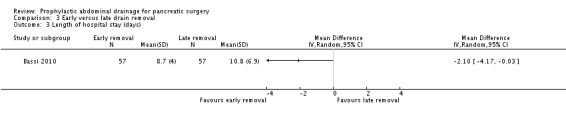
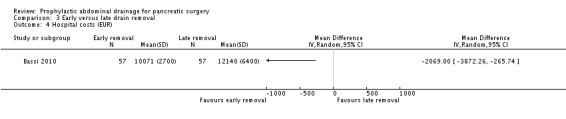
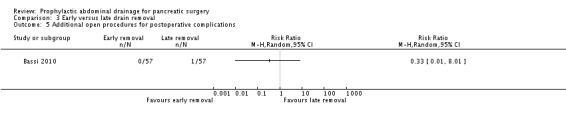
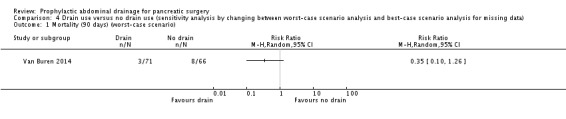
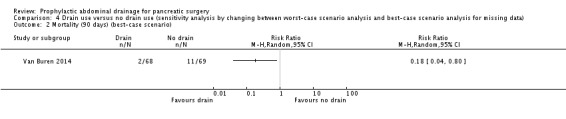
Main results: Drain use versus no drain useWe included three trials involving 711 participants who were randomized to the drainage group (N = 358) and the no drainage group (N = 353) after pancreatic surgery. There was inadequate evidence to establish the effect of drains on mortality at 30 days (2.2% with drains versus 3.4% no drains; RR 0.78, 95% CI 0.31 to 1.99; three studies; low-quality evidence), mortality at 90 days (2.9% versus 11.6%; RR 0.24, 95% CI 0.05 to 1.10; one study; low-quality evidence), intra-abdominal infection (7.3% versus 8.5%; RR 0.89, 95% CI 0.36 to 2.20; three studies; very low-quality evidence), wound infection (12.3% versus 13.3%; RR 0.92, 95% CI 0.63 to 1.36; three studies; low-quality evidence), morbidity (64.8% versus 62.0%; RR 1.04, 95% CI 0.93 to 1.16; three studies; moderate-quality evidence), length of hospital stay (MD -0.66 days, 95% CI -1.60 to 0.29; three studies; moderate-quality evidence), or additional open procedures for postoperative complications (11.5% versus 9.1%; RR 1.18, 95% CI 0.55 to 2.52; three studies). There was one drain-related complication in the drainage group (0.6%). Type of drainWe included one trial involving 160 participants who were randomized to the active drain group (N = 82) and the passive drain group (N = 78) after pancreatic surgery. There was no evidence of differences between the two groups in mortality at 30 days (1.2% with active drain versus 0% with passive drain), intra-abdominal infection (0% versus 2.6%), wound infection (6.1% versus 9.0%; RR 0.68, 95% CI 0.23 to 2.05), morbidity (22.0% versus 32.1%; RR 0.68, 95% CI 0.41 to 1.15), or additional open procedures for postoperative complications (1.2% versus 7.7%; RR 0.16, 95% CI 0.02 to 1.29). The active drain group was associated with shorter length of hospital stay (MD -1.90 days, 95% CI -3.67 to -0.13; 14.1% decrease of an 'average' length of hospital stay) than in the passive drain group. The quality of evidence was low, or very low. Early versus late drain removalWe included one trial involving 114 participants with a low risk of postoperative pancreatic fistula who were randomized to the early drain removal group (N = 57) and the late drain removal group (N = 57) after pancreatic surgery. There was no evidence of differences between the two groups in mortality at 30 days (0% for both groups) or additional open procedures for postoperative complications (0% with early drain removal versus 1.8% with late drain removal; RR 0.33, 95% CI 0.01 to 8.01). The early drain removal group was associated with lower rates of postoperative complications (38.5% versus 61.4%; RR 0.63, 95% CI 0.43 to 0.93), shorter length of hospital stay (MD -2.10 days, 95% CI -4.17 to -0.03; 21.5% decrease of an 'average' length of hospital stay), and hospital costs (17.0% decrease of 'average' hospital costs) than in the late drain removal group. The quality of evidence for each of the outcomes was low.
Authors' conclusions: It is unclear whether routine abdominal drainage has any effect on the reduction of mortality and postoperative complications after pancreatic surgery. In case of drain insertion, low-quality evidence suggests that active drainage may reduce hospital stay after pancreatic surgery, and early removal may be superior to late removal for people with low risk of postoperative pancreatic fistula.
Conflict of interest statement
YC: none known.
JX: none known.
ML: none known.
NC: none known.
SH: none known.
Figures

Update of
-
Prophylactic abdominal drainage for pancreatic surgery.Cochrane Database Syst Rev. 2015 Aug 21;(8):CD010583. doi: 10.1002/14651858.CD010583.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2016 Oct 21;10:CD010583. doi: 10.1002/14651858.CD010583.pub3. PMID: 26292656 Updated.
References
References to studies included in this review
-
- Bassi C, Molinari E, Malleo G, Crippa S, Butturini G, Salvia R, et al. Early versus late drain removal after standard pancreatic resections: results of a prospective randomized trial. Annals of Surgery 2010;252(2):207‐14. [] - PubMed
-
2864182
-
- Jiang H, Liu N, Zhang M, Lu L, Dou R, Qu L. A randomized trial on the efficacy of prophylactic active drainage in prevention of complications after pancreaticoduodenectomy. Scandinavian Journal of Surgery 2016;1(1):1457496916665543. [] - PubMed
-
4439016
-
- McMillan MT, Fisher WE, Buren G, McElhany A, Bloomston M, Hughes SJ, et al. The value of drains as a fistula mitigation strategy for pancreatoduodenectomy: something for everyone? Results of a randomized prospective multi‐institutional study. Journal of Gastrointestinal Surgery 2015;19(1):21‐30. [] - PubMed
- McMillan MT, Malleo G, Bassi C, Butturini G, Salvia R, Roses RE, et al. Drain management after pancreatoduodenectomy: reappraisal of a prospective randomized trial using risk stratification. Journal of the American College of Surgeons 2015;221(4):798‐809. [] - PubMed
- Buren G, Bloomston M, Hughes SJ, Winter J, Behrman SW, Zyromski NJ, et al. A randomized prospective multicenter trial of pancreaticoduodenectomy with and without routine intraperitoneal drainage. Annals of Surgery 2014;259(4):605‐12. [] - PubMed
-
2864186
-
- Witzigmann H, Diener M K, Kienkötter S, Rossion I, Bruckner T, Werner B, et al. No need for routine drainage after pancreatic head resection: the dual‐center, randomized, controlled PANDRA trial (ISRCTN04937707). Annals of Surgery 2016;264(3):528‐37. [] - PubMed
-
4439020
References to studies excluded from this review
-
- Adham M, Chopin‐Laly X, Lepilliez V, Gincul R, Valette PJ, Ponchon T. Pancreatic resection: drain or no drain?. Surgery 2013;154(5):1069‐77. [] - PubMed
-
2864188
-
- Giovinazzo F, Butturini G, Salvia R, Mascetta G, Monsellato D, Marchegiani G, et al. Drain management after pancreatic resection: state of the art. Journal of Hepato‐Biliary‐Pancreatic Sciences 2011;18(6):779‐84. [] - PubMed
-
2864194
References to ongoing studies
Additional references
-
- Allen PJ, Gönen M, Brennan MF, Bucknor AA, Robinson LM, Pappas MM, et al. Pasireotide for postoperative pancreatic fistula. New England Journal of Medicine 2014;370(21):2014‐22. - PubMed
-
- Anderson KE, Mack T, Silverman D. Cancer of the pancreas. In: Schottenfeld D, Fraumeni JF Jr editor(s). Cancer Epidemiology and Prevention. 3rd Edition. New York: Oxford University Press, 2006:1‐1416.
-
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138(1):8‐13. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous