

Individualized prophylaxis for optimizing hemophilia care: can we apply this to both developed and developing nations?
- PMID: 27766058
- PMCID: PMC5056486
- DOI: 10.1186/s12959-016-0096-y
Individualized prophylaxis for optimizing hemophilia care: can we apply this to both developed and developing nations?
Abstract
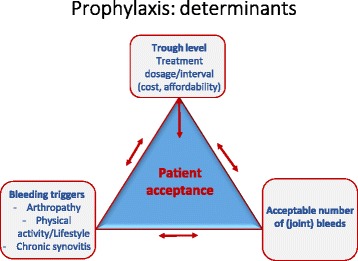
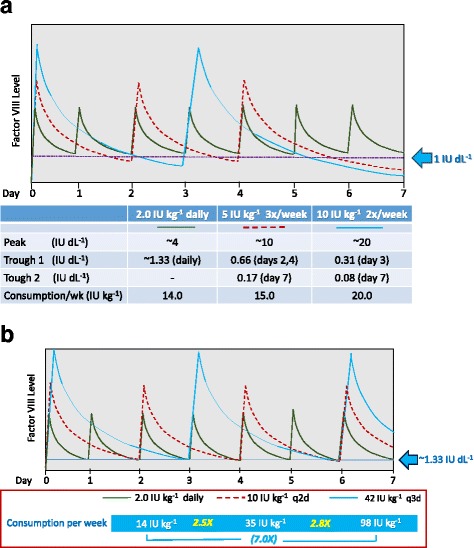
Prophylaxis is considered optimal care for hemophilia patients to prevent bleeding and to preserve joint function thereby improving quality of life (QoL). The evidence for prophylaxis is irrefutable and is the standard of care in developed nations. Prophylaxis can be further individualized to improve outcomes and cost effectiveness. Individualization is best accomplished taking into account the bleeding phenotype, physical activity/lifestyle, joint status, and pharmacokinetic handling of specific clotting factor concentrates, all of which vary among individuals. Patient acceptance should also be considered. Assessment tools (e.g. joint status imaging and function studies/scores, QoL) for determining and monitoring risk factors and outcome, as well as population PK profiling have been developed to assist the individualization process. The determinants of optimal prophylaxis include (1) factor dose/dosing frequency, hence, cost/affordability (2) bleeding triggers (physical activity/lifestyle, chronic arthropathy and synovitis) and (3) bleeding rates. Altering one determinant results in adjustment of the other two. Thus, the trough level to protect from spontaneous bleeding can be increased in patients who have greater bleeding risks; and prophylaxis to achieve zero joint bleeds is achievable through optimal individualization. Prophylaxis in economically constrained nations is limited by the ill-affordability of clotting factor concentrates. However, at least 5 studies on children and adults from Thailand, China and India have shown superiority of low dose (~5-10 IU kg-1 2-3× per week) prophylaxis over episodic treatment in terms of bleed reduction, and quality of life, with improved physical activity, independent functioning, school attendance and community participation. In these nations, the prophylaxis goals should be for improved QoL rather than "zero bleeds" and perfect joints. Prophylaxis can still be individualized to affordability. Higher protective trough level can be achieved by using smaller doses given more frequently without an increase in consumption/cost. The bleeding trigger can also be down-regulated by avoiding unnecessary injury, and by engaging in judicious strengthening exercises appropriate to the joint status to improve balance and joint stabilization. Central to the success of prophylaxis are clinics with comprehensive care that provide the necessary professional expertise, support, and counseling, to educate patients, families, and other healthcare professionals, and to support research for improved hemophilia care.
Keywords: Hemophilia; Individualized prophylaxis; Low-dose prophylaxis; Personalized prophylaxis; Pharmacokinetics; Population pharmacokinetics; Terminal half-life.
Figures
Similar articles
-
Significant reduction in hemarthrosis in boys with severe hemophilia A: The China hemophilia individualized low-dose secondary prophylaxis study.Res Pract Thromb Haemost. 2021 Sep 18;5(6):e12552. doi: 10.1002/rth2.12552. eCollection 2021 Aug. Res Pract Thromb Haemost. 2021. PMID: 34568725 Free PMC article.
-
Individualizing prophylaxis in hemophilia: a review.Expert Rev Hematol. 2015 Apr;8(2):237-46. doi: 10.1586/17474086.2015.1002465. Epub 2015 Jan 20. Expert Rev Hematol. 2015. PMID: 25600578 Review.
-
Defining the impact of hemophilia: the Academic Achievement in Children with Hemophilia Study.Pediatrics. 2001 Dec;108(6):E105. doi: 10.1542/peds.108.6.e105. Pediatrics. 2001. PMID: 11731632
-
[Efficacy of short-term full-dose prophylaxis in adult Chinese patients with severe hemophilia A].Nan Fang Yi Ke Da Xue Xue Bao. 2018 Sep 30;38(10):1222-1227. doi: 10.3969/j.issn.1673-4254.2018.10.11. Nan Fang Yi Ke Da Xue Xue Bao. 2018. PMID: 30377129 Free PMC article. Chinese.
-
Prophylaxis in real life scenarios.Haemophilia. 2014 May;20 Suppl 4:106-13. doi: 10.1111/hae.12425. Haemophilia. 2014. PMID: 24762285 Review.
Cited by
-
A Real-World Analysis of Commonly Prescribed FVIII Products Based on U.S. Medical Charts: Consumption and Bleeding Outcomes in Hemophilia A Patients.J Manag Care Spec Pharm. 2020 Oct;26(10):1258-1265. doi: 10.18553/jmcp.2020.20199. Epub 2020 Aug 21. J Manag Care Spec Pharm. 2020. PMID: 32820685 Free PMC article.
-
Target joint resolution in patients with haemophilia A receiving long-term prophylaxis with BAY 94-9027.Haemophilia. 2020 Jul;26(4):e201-e204. doi: 10.1111/hae.13982. Epub 2020 Jun 23. Haemophilia. 2020. PMID: 32578323 Free PMC article. No abstract available.
-
The role of patient and healthcare professionals in the era of new hemophilia treatments in developed and developing countries.Ther Adv Hematol. 2018 Jul 2;9(8):239-249. doi: 10.1177/2040620718784830. eCollection 2018 Aug. Ther Adv Hematol. 2018. PMID: 30181844 Free PMC article. Review.
-
Modeling of Body Weight Metrics for Effective and Cost-Efficient Conventional Factor VIII Dosing in Hemophilia A Prophylaxis.Pharmaceutics. 2017 Oct 17;9(4):47. doi: 10.3390/pharmaceutics9040047. Pharmaceutics. 2017. PMID: 29039750 Free PMC article.
-
Nonacog beta pegol (N9-GP) in hemophilia B: First report on safety and efficacy in previously untreated and minimally treated patients.Res Pract Thromb Haemost. 2020 Jul 29;4(7):1101-1113. doi: 10.1002/rth2.12412. eCollection 2020 Oct. Res Pract Thromb Haemost. 2020. PMID: 33134776 Free PMC article.
References
-
- Manco-Johnson MJ, Kempton CL, Reding MT, Lissitchkov T, Goranov S, Gercheva L, et al. Randomized, controlled, parallel-group trial of routine prophylaxis vs. on-demand treatment with sucrose-formulated recombinant factor VIII in adults with severe hemophilia A. J Thromb Haemost. 2013;11:1119–27. doi: 10.1111/jth.12202. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
