

Review
doi: 10.1186/s13017-016-0105-2.
eCollection 2016.
WSES classification and guidelines for liver trauma
Affiliations
- PMID: 27766112
- PMCID: PMC5057434
- DOI: 10.1186/s13017-016-0105-2
Item in Clipboard
Review
WSES classification and guidelines for liver trauma
World J Emerg Surg.
.
Abstract
The severity of liver injuries has been universally classified according to the American Association for the Surgery of Trauma (AAST) grading scale. In determining the optimal treatment strategy, however, the haemodynamic status and associated injuries should be considered. Thus the management of liver trauma is ultimately based on the anatomy of the injury and the physiology of the patient. This paper presents the World Society of Emergency Surgery (WSES) classification of liver trauma and the management Guidelines.
Keywords: Classification; Guidelines; Hemorrage; Liver trauma; Minor; Moderate; Non-operative management; Operative management; Severe; Surgery.
Figures
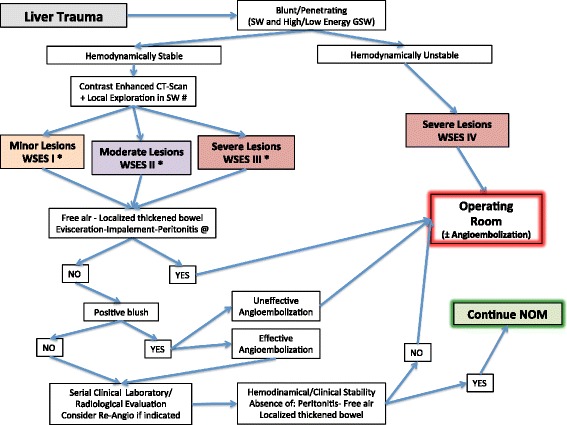
Liver Trauma Management Algorithm. (SW Stab Wound, GSW Gun Shot Wound; *NOM should only be attempted in centers capable of a precise diagnosis of the severity of liver injuries and capable of intensive management (close clinical observation and haemodynamic monitoring in a high dependency/intensive care environment, including serial clinical examination and laboratory assay, with immediate access to diagnostics, interventional radiology and surgery and immediately available access to blood and blood products; # wound exploration near the inferior costal margin should be avoided if not strictly necessary because of the high risk to damage the intercostal vessels; @ extremely selected patients hemodynamically stable with evisceration and/or impalement and/or diffuse peritonitis with the certainty of an exclusive and isolated abdominal lesion could be considered as candidate to be directly taken to the operating room without contrast enanched CT-scan)
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
