

Quantifying Quadriceps Muscle Strength in Patients With ACL Injury, Focal Cartilage Lesions, and Degenerative Meniscus Tears: Differences and Clinical Implications
- PMID: 27766275
- PMCID: PMC5063093
- DOI: 10.1177/2325967116667717
Quantifying Quadriceps Muscle Strength in Patients With ACL Injury, Focal Cartilage Lesions, and Degenerative Meniscus Tears: Differences and Clinical Implications
Abstract
Background: Reduced quadriceps strength influences knee function and increases the risk of knee osteoarthritis. Thus, it is of significant clinical relevance to precisely quantify strength deficits in patients with knee injuries.
Purpose: To evaluate isokinetic concentric quadriceps muscle strength torque values, assessed both from peak torque and at specific knee flexion joint angles, in patients with anterior cruciate ligament (ACL) injury, focal cartilage lesions, and degenerative meniscus tears.
Study design: Cohort study; Level of evidence, 3.
Methods: Data were synthesized from patients included in 3 previously conducted research projects: 2 prospective cohort studies and 1 randomized controlled trial. At the time of inclusion, all patients were candidates for surgery. Isokinetic concentric quadriceps muscle strength measurements (60 deg/s) were performed at baseline (preoperative status) and after a period of progressive supervised exercise therapy (length of rehabilitation period: 5 weeks for ACL injury, 12 weeks for cartilage lesions and degenerative meniscus). Outcome measures were peak torque and torque at specific knee flexion joint angles from 20° to 70°. All patients had unilateral injuries, and side-to-side deficits were calculated. For comparisons between and within groups, we utilized 1-way analysis of variance and paired t tests, respectively.
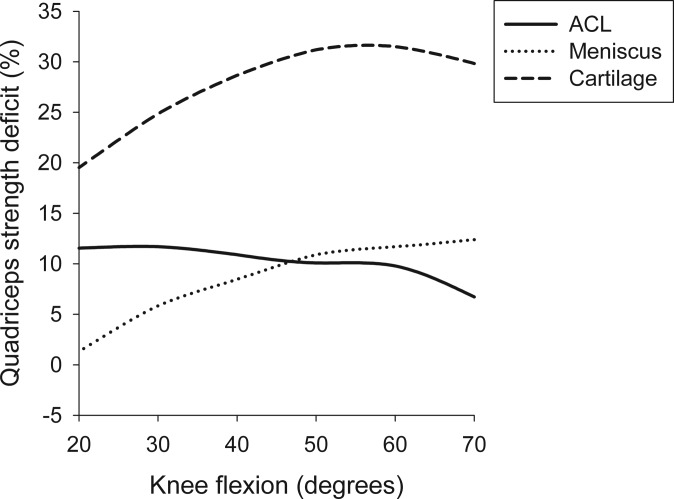
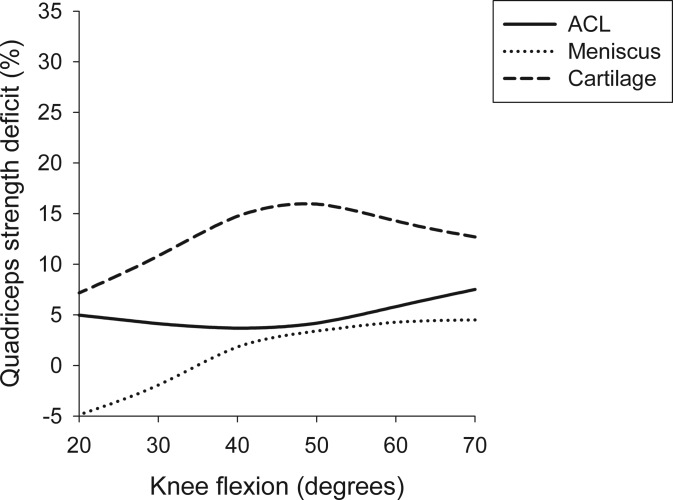
Results: In total, 250 patients were included. At baseline, cartilage patients had the most severe deficit (39.7% ± 24.3%; P < .001). Corresponding numbers for ACL and degenerative meniscus subjects were 21.7% (±13.2%) and 20.7% (±16.3%), respectively. At retest, there was significant improvement in all groups (P < .001), with remaining deficits of 24.7% (±18.5%) for cartilage, 16.8% (±13.9%) for ACL, and 3.3% (±17.8%) for degenerative meniscus. Peak torque was consistently measured at 60° of knee flexion, whereas the largest mean deficits were measured at 30° at baseline and 70° at retest for the ACL group, at 70° at baseline and retest for the degenerative meniscus group, and at 60° at baseline and at 50° at retest for the cartilage group.
Conclusion: This study underlines the importance of including torque at specific knee flexion joint angles from isokinetic assessments to identify the most severe quadriceps muscle strength deficits. Furthermore, it confirms the importance of progressive exercise therapy interventions before potential surgery in patients with knee injuries.
Keywords: ACL; articular cartilage; knee; meniscus; physical therapy/rehabilitation.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This study is based on funding from the following grants: The Delaware-Oslo ACL Cohort (NIH Grant No. 5 R37 HD 037985 -11); the OMEX study: The South-Eastern Norway Regional Health Authority, Sophies Minde Ortopedi AS, the Swedish Rheumatism Association, the Swedish Scientific Council, Region of Southern Denmark, and the Danish Rheumatism Association; and the Oslo CARE study: South-Eastern Norway Regional Health Authority and the Norwegian Research Council. The OMEX study is registered on Clinicaltrials.gov: NCT01002794.
Figures
References
-
- Blackburn JT, Pamukoff DN, Sakr M, Vaughan AJ, Berkoff DJ. Whole body and local muscle vibration reduce artificially induced quadriceps arthrogenic inhibition. Arch Phys Med Rehabil. 2014;95:2021–2028. - PubMed
-
- Carpenter MR, Carpenter RL, Peel J, et al. The reliability of isokinetic and isometric leg strength measures among individuals with symptoms of mild osteoarthritis. J Sports Med Phys Fitness. 2006;46:585–589. - PubMed
-
- de Valk EJ, Moen MH, Winters M, Bakker EW, Tamminga R, van der Hoeven H. Preoperative patient and injury factors of successful rehabilitation after anterior cruciate ligament reconstruction with single-bundle techniques. Arthroscopy. 2013;29:1879–1895. - PubMed
-
- Dvir Z. Isokinetics: Muscle Testing, Interpretation and Clinical Applications. New York: Churchill Livingstone; 1995.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
