

Ambulatory Pediatric Surveillance of Hand, Foot and Mouth Disease as Signal of an Outbreak of Coxsackievirus A6 Infections, France, 2014-2015
- PMID: 27767012
- PMCID: PMC5088007
- DOI: 10.3201/eid2211.160590
Ambulatory Pediatric Surveillance of Hand, Foot and Mouth Disease as Signal of an Outbreak of Coxsackievirus A6 Infections, France, 2014-2015
Abstract
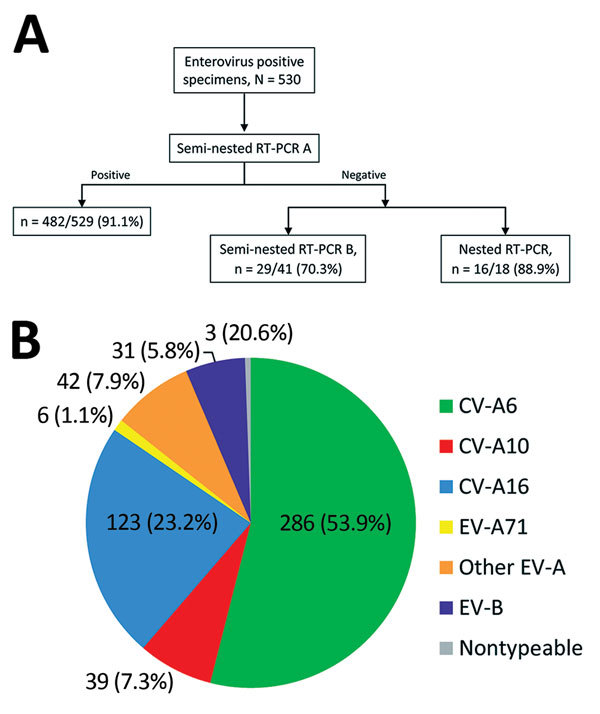
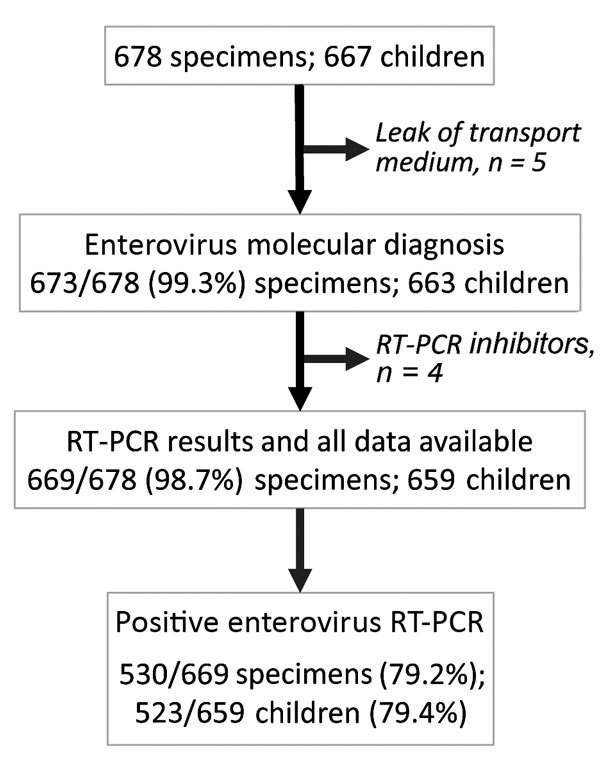
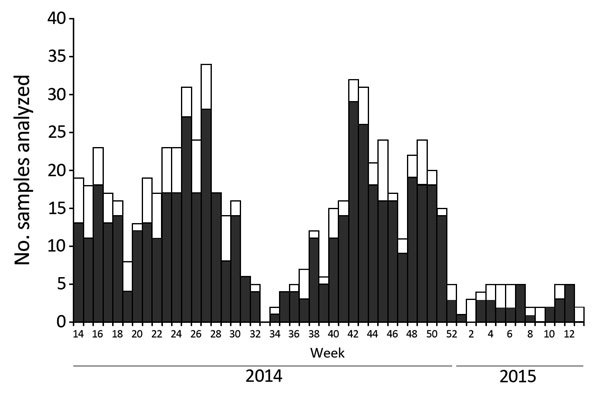
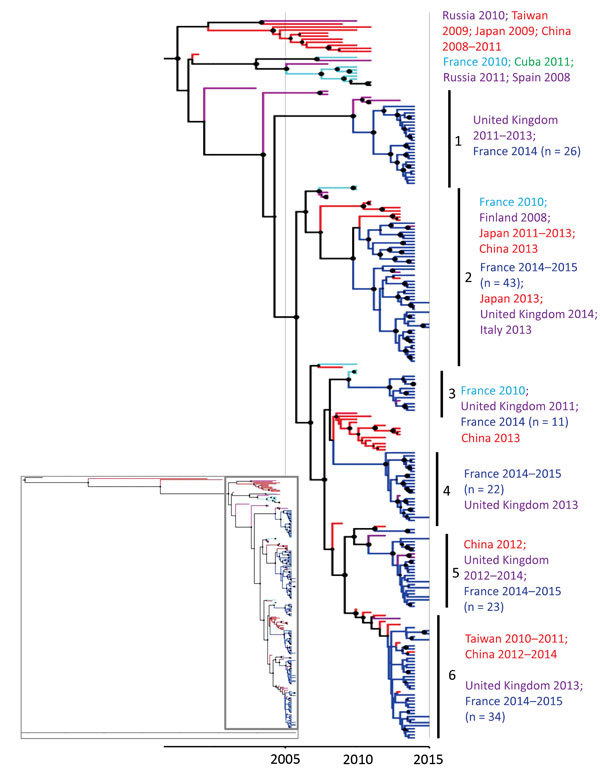
The clinical impact of enteroviruses associated with hand, foot and mouth disease (HFMD) is unknown outside Asia, and the prevalence of enterovirus A71 (EV-A71) in particular might be underestimated. To investigate the prevalence of enterovirus serotypes and the clinical presentations associated with HFMD in France, we conducted prospective ambulatory clinic-based surveillance of children during April 2014-March 2015. Throat or buccal swabs were collected from children with HFMD and tested for the enterovirus genome. Physical examinations were recorded on a standardized form. An enterovirus infection was detected in 523 (79.3%) of 659 children tested. Two epidemic waves occurred, dominated by coxsackievirus (CV) A6, which was detected in 53.9% of enterovirus-infected children. CV-A6 was more frequently related to atypical HFMD manifestations (eruptions extended to limbs and face). Early awareness and documentation of HFMD outbreaks can be achieved by syndromic surveillance of HFMD by ambulatory pediatricians and rapid enterovirus testing and genotyping.
Keywords: France; ambulatory; enterovirus A; foot and mouth disease; hand; human coxsackievirus infections; pediatric; sentinel surveillance; surveillance viruses.
Figures
References
-
- Messacar K, Schreiner TL, Maloney JA, Wallace A, Ludke J, Oberste MS, et al. A cluster of acute flaccid paralysis and cranial nerve dysfunction temporally associated with an outbreak of enterovirus D68 in children in Colorado, USA. Lancet. 2015;385:1662–71. 10.1016/S0140-6736(14)62457-0 - DOI - PubMed
-
- World Health Organization. Enterovirus surveillance guidelines: guidelines for enterovirus surveillance in support of the Polio Eradication Initiative. Geneva: The Organization; 2015. [cited 2015 Apr 2]. http://www.euro.who.int/en/publications/abstracts/enterovirus-surveillan...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
