

Association of Kidney Function Biomarkers with Brain MRI Findings: The BRINK Study
- PMID: 27767995
- PMCID: PMC5621389
- DOI: 10.3233/JAD-160834
Association of Kidney Function Biomarkers with Brain MRI Findings: The BRINK Study
Abstract
Background: Chronic kidney disease (CKD) studies have reported variable prevalence of brain pathologies, in part due to low inclusion of participants with moderate to severe CKD.
Objective: To measure the association between kidney function biomarkers and brain MRI findings in CKD.
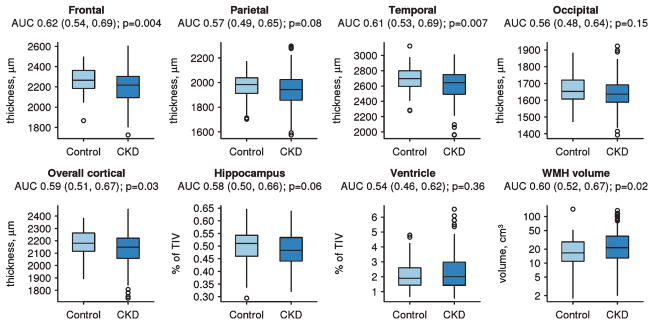
Methods: In the BRINK (BRain IN Kidney Disease) study, MRI was used to measure gray matter volumes, cerebrovascular pathologies (white matter hyperintensity (WMH), infarctions, microhemorrhages), and microstructural changes using diffusion tensor imaging (DTI). We performed regression analyses with estimated glomerular filtration rate (eGFR) and urine albumin to creatinine ratio (UACR) as primary predictors, and joint models that included both predictors, adjusted for vascular risk factors.
Results: We obtained 240 baseline MRI scans (150 CKD with eGFR <45 in ml/min/1.73 m2; 16 mild CKD: eGFR 45-59; 74 controls: eGFR≥60). Lower eGFR was associated with greater WMH burden, increased odds of cortical infarctions, and worsening diffusion changes throughout the brain. In eGFR models adjusted for UACR, only cortical infarction associations persisted. However, after adjusting for eGFR, higher UACR provided additional information related to temporal lobe atrophy, increased WMH, and whole brain microstructural changes as measured by increased DTI mean diffusivity.
Conclusions: Biomarkers of kidney disease (eGFR and UACR) were associated with MRI brain changes, even after accounting for vascular risk factors. UACR adds unique additional information to eGFR regarding brain structural and diffusion biomarkers. There was a greater impact of kidney function biomarkers on cerebrovascular pathologies and microstructural brain changes, suggesting that cerebrovascular etiology may be the primary driver of cognitive impairment in CKD.
Keywords: Cerebrovascular disease; chronic kidney disease; infarctions; magnetic resonance imaging.
Figures


References
-
- Seliger SL, Siscovick DS, Stehman-Breen CO, Gillen DL, Fitzpatrick A, Bleyer A, Kuller LH. Moderate renal impairment and risk of dementia among older adults: The Cardiovascular Health Cognition Study. J Am Soc Nephrol. 2004;15:1904–1911. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
