

An independent validation of a gene expression signature to differentiate malignant melanoma from benign melanocytic nevi
- PMID: 27768230
- PMCID: PMC5324582
- DOI: 10.1002/cncr.30385
An independent validation of a gene expression signature to differentiate malignant melanoma from benign melanocytic nevi
Abstract
Background: Recently, a 23-gene signature was developed to produce a melanoma diagnostic score capable of differentiating malignant and benign melanocytic lesions. The primary objective of this study was to independently assess the ability of the gene signature to differentiate melanoma from benign nevi in clinically relevant lesions.
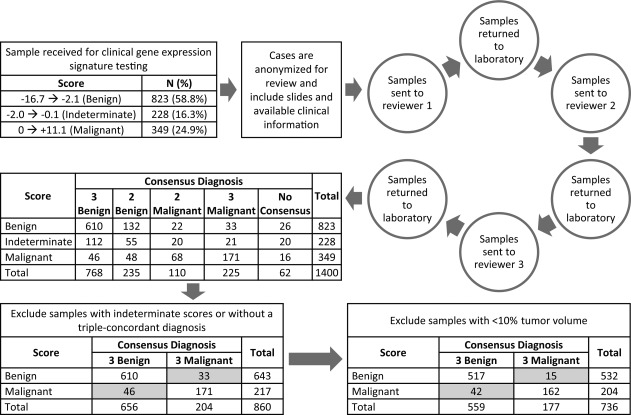
Methods: A set of 1400 melanocytic lesions was selected from samples prospectively submitted for gene expression testing at a clinical laboratory. Each sample was tested and subjected to an independent histopathologic evaluation by 3 experienced dermatopathologists. A primary diagnosis (benign or malignant) was assigned to each sample, and diagnostic concordance among the 3 dermatopathologists was required for inclusion in analyses. The sensitivity and specificity of the score in differentiating benign and malignant melanocytic lesions were calculated to assess the association between the score and the pathologic diagnosis.
Results: The gene expression signature differentiated benign nevi from malignant melanoma with a sensitivity of 91.5% and a specificity of 92.5%.
Conclusions: These results reflect the performance of the gene signature in a diverse array of samples encountered in routine clinical practice. Cancer 2017;123:617-628. © 2016 American Cancer Society.
Keywords: clinical validation; gene expression; melanoma; molecular diagnosis; reverse transcription-polymerase chain reaction.
© 2016 Myriad Genetics, Inc. Cancer published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Figures




References
-
- American Cancer Society . Cancer Facts & Figures 2015. Atlanta, GA: American Cancer Society; 2015.
-
- American Cancer Society . What are the survival rates for melanoma skin cancer by stage? http://www.cancer.org/cancer/skincancer-melanoma/detailedguide/melanoma-.... Accessed January 21, 2016.
-
- Shoo BA, Sagebiel RW, Kashani‐Sabet M. Discordance in the histopathologic diagnosis of melanoma at a melanoma referral center. J Am Acad Dermatol. 2010;62:751–756. - PubMed
-
- Hawryluk EB, Sober AJ, Piris A, et al. Histologically challenging melanocytic tumors referred to a tertiary care pigmented lesion clinic. J Am Acad Dermatol. 2012;67:727–735. - PubMed
-
- Veenhuizen KC, De Wit PE, Mooi WJ, Scheffer E, Verbeek AL, Ruiter DJ. Quality assessment by expert opinion in melanoma pathology: experience of the pathology panel of the Dutch Melanoma Working Party. J Pathol. 1997;182:266–272. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
