

Computed Tomographic Appearance of Organizing Pneumonia in an Oncologic Patient Population
- PMID: 27768620
- PMCID: PMC5469368
- DOI: 10.1097/RCT.0000000000000520
Computed Tomographic Appearance of Organizing Pneumonia in an Oncologic Patient Population
Abstract
Objective: The aims of this study were to describe the computed tomographic features of organizing pneumonia (OP) in an oncologic patient population and to also identify features associated with lung cancer and patients undergoing hematopoietic stem cell transplant (HSCT).
Methods: In retrospective computed tomographies from 151 patients with pathologically confirmed OP between January 2009 and September 2014, number of lesions, location, size, margin type, and consistency, as well as volume of lymphadenopathy and the presence and size of pleural effusions, were recorded. Associated malignancy was noted.
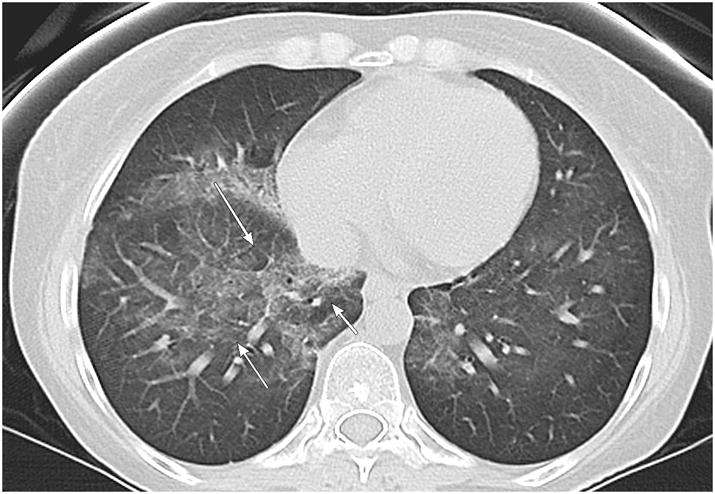
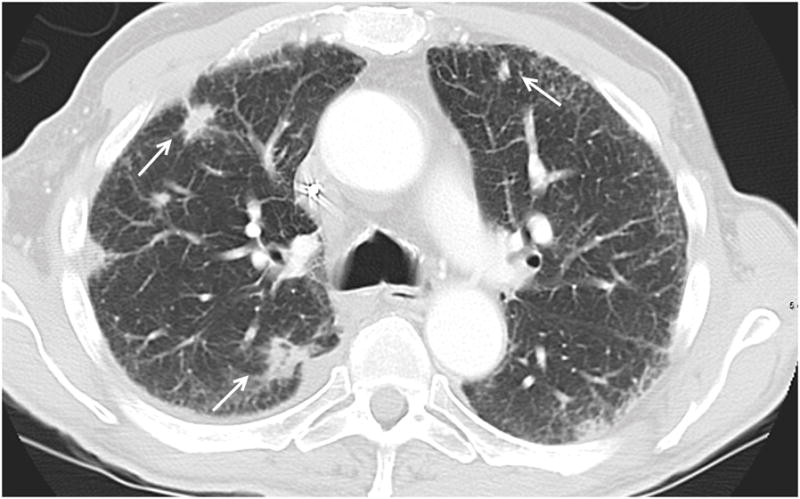
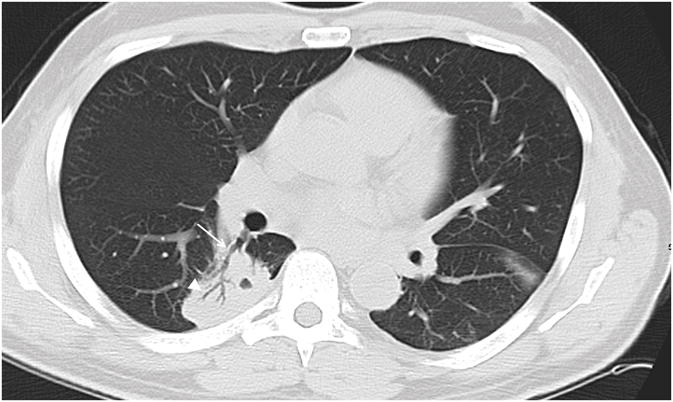
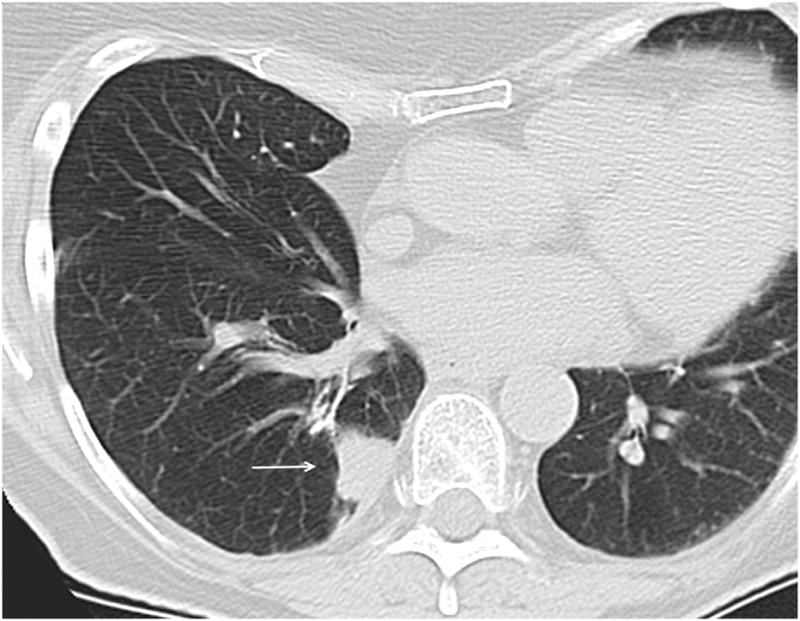
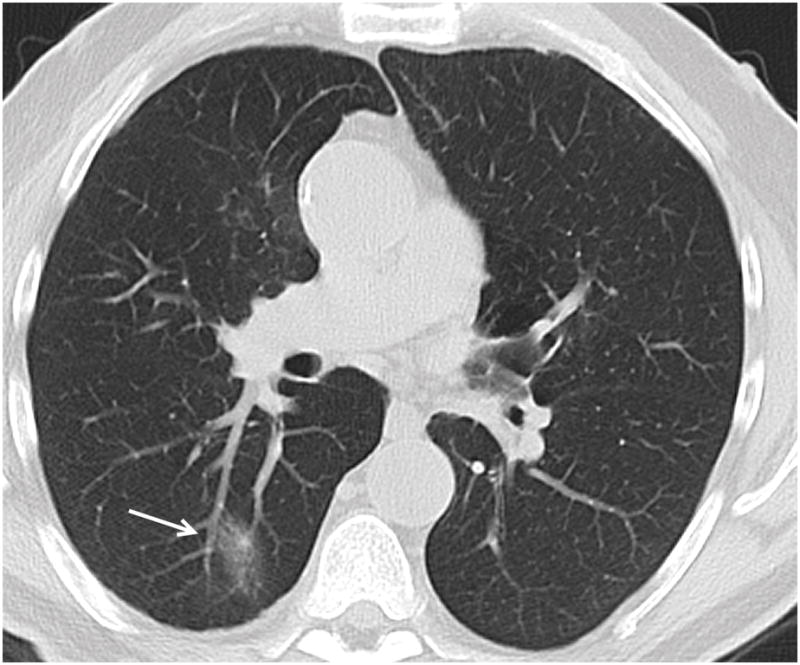
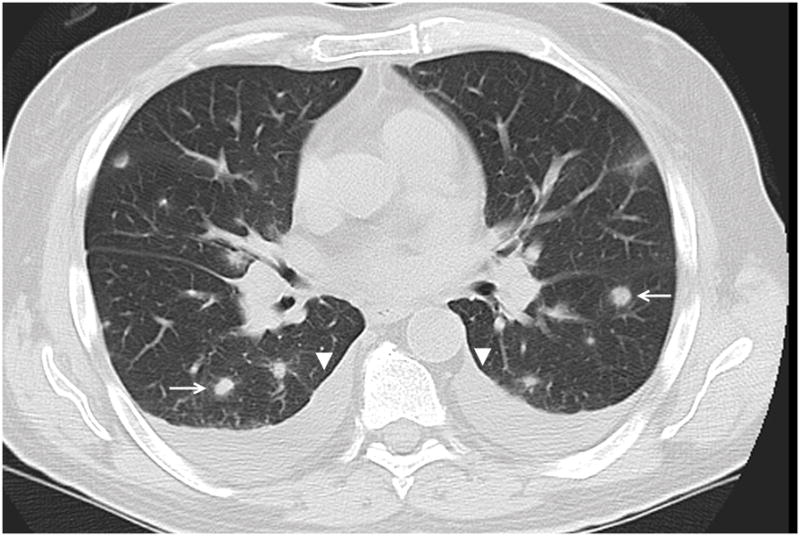
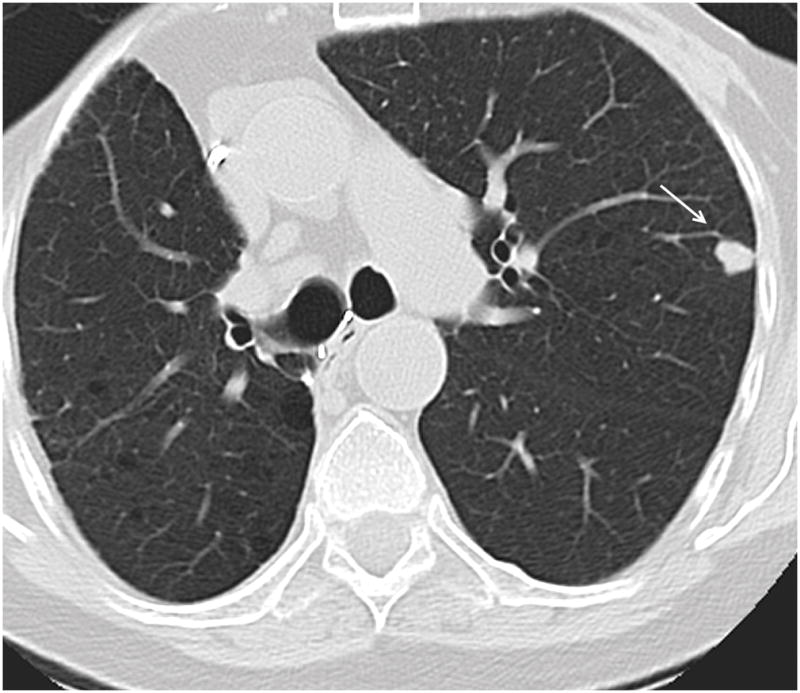
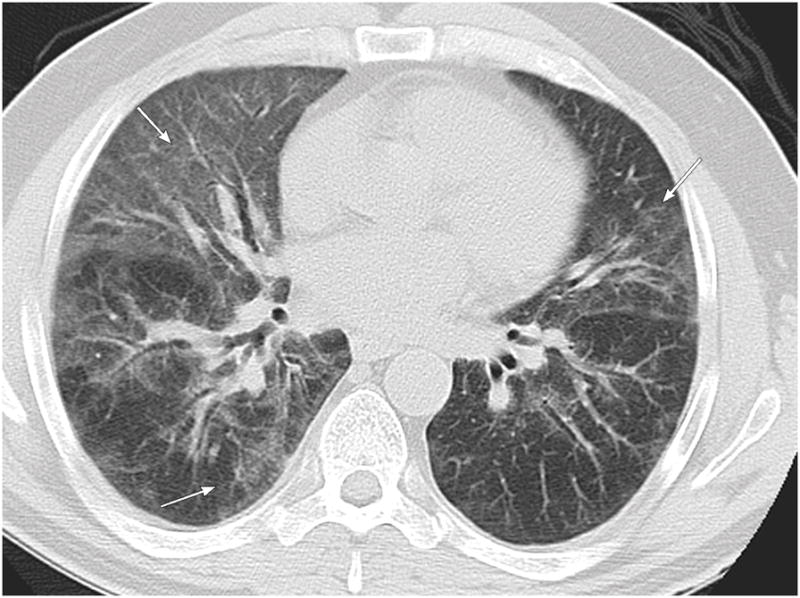
Results: Organizing pneumonia most commonly presented as a diffuse process (n = 62, 41%), frequently occupied both a central and peripheral location (n = 79, 53%), and commonly presented with a solid appearance (n = 67, 44%) or with ground glass opacity (n = 80, 53%). Pleural effusions were seen in 68 patients (45%). Organizing pneumonia less frequently contained air bronchograms, cavitation, necrosis, surrounding ground glass opacity, or adjacent bronchiectasis. In patients with lung cancer (n = 25, 17%), OP more likely presented as discrete lesions and occupied a peripheral location as compared with patients with other malignancies (Ps = 0.025 and 0.002). In HSCT patients (n = 29, 19%), a diffuse process was more commonly seen than in non-HSCT patients (P = 0.038).
Conclusions: Organizing pneumonia more commonly presents as discrete lesions with a peripheral location in patients with lung cancer and as a diffuse process in patients who had undergone HSCT.
Conflict of interest statement
Figures
References
-
- Zhao F, Yan SX, Wang GF, et al. CT features of focal organizing pneumonia: an analysis of consecutive histopathologically confirmed 45 cases. Eur J Radiol. 2014;83:73–8. - PubMed
-
- Miao L, Wang Y, Li Y, et al. Lesion with morphologic feature of organizing pneumonia (OP) in CT-guided lung biopsy samples for diagnosis of bronchiolitis obliterans organizing pneumonia (BOOP): a retrospective study of 134 cases in a single center. Journal of thoracic disease. 2014;6:1251–60. - PMC - PubMed
-
- Mueller-Mang C, Grosse C, Schmid K, et al. What every radiologist should know about idiopathic interstitial pneumonias. Radiographics : a review publication of the Radiological Society of North America, Inc. 2007;27:595–615. - PubMed
-
- Cordier JF, Loire R, Brune J. Idiopathic bronchiolitis obliterans organizing pneumonia. Definition of characteristic clinical profiles in a series of 16 patients. Chest. 1989;96:999–1004. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
