

Assessing the burden of medical impoverishment by cause: a systematic breakdown by disease in Ethiopia
- PMID: 27769296
- PMCID: PMC5075208
- DOI: 10.1186/s12916-016-0697-0
Assessing the burden of medical impoverishment by cause: a systematic breakdown by disease in Ethiopia
Abstract
Background: Out-of-pocket (OOP) medical expenses often lead to catastrophic expenditure and impoverishment in low- and middle-income countries. Yet, there has been no systematic examination of which specific diseases and conditions (e.g., tuberculosis, cardiovascular disease) drive medical impoverishment, defined as OOP direct medical costs pushing households into poverty.
Methods: We used a cost and epidemiological model to propose an assessment of the burden of medical impoverishment in Ethiopia, i.e., the number of households crossing a poverty line due to excessive OOP direct medical expenses. We utilized disease-specific mortality estimates from the Global Burden of Disease study, epidemiological and cost inputs from surveys, and secondary data from the literature to produce a count of poverty cases due to OOP direct medical costs per specific condition.
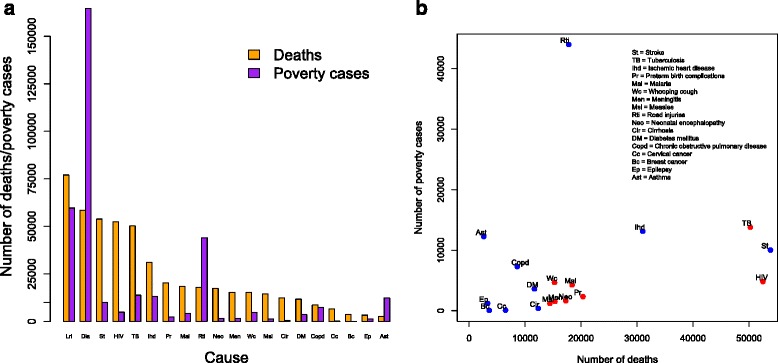
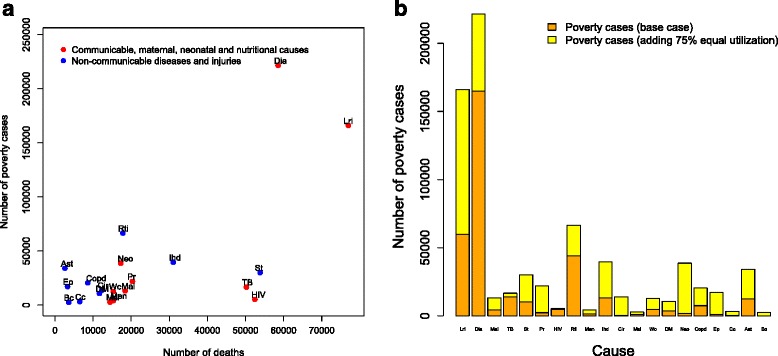
Results: In Ethiopia, in 2013, and among 20 leading causes of mortality, we estimated the burden of impoverishment due to OOP direct medical costs to be of about 350,000 poverty cases. The top three causes of medical impoverishment were diarrhea, lower respiratory infections, and road injury, accounting for 75 % of all poverty cases.
Conclusions: We present a preliminary attempt for the estimation of the burden of medical impoverishment by cause for high mortality conditions. In Ethiopia, medical impoverishment was notably associated with illness occurrence and health services utilization. Although currently used estimates are sensitive to health services utilization, a systematic breakdown of impoverishment due to OOP direct medical costs by cause can provide important information for the promotion of financial risk protection and equity, and subsequent design of health policies toward universal health coverage, reduction of direct OOP payments, and poverty alleviation.
Keywords: Catastrophic health expenditure; Direct medical payments; Ethiopia; Financial risk protection; Medical impoverishment; Out-of-pocket costs; Poverty.
Figures

Similar articles
-
Assessing medical impoverishment and associated factors in health care in Ethiopia.BMC Int Health Hum Rights. 2020 Mar 30;20(1):7. doi: 10.1186/s12914-020-00227-x. BMC Int Health Hum Rights. 2020. PMID: 32228634 Free PMC article.
-
Catastrophic healthcare expenditure and impoverishment in tropical deltas: evidence from the Mekong Delta region.Int J Equity Health. 2018 Apr 27;17(1):53. doi: 10.1186/s12939-018-0757-5. Int J Equity Health. 2018. PMID: 29703209 Free PMC article.
-
Catastrophic health expenditure and impoverishment in households of persons with depression: a cross-sectional, comparative study in rural Ethiopia.BMC Public Health. 2019 Jul 11;19(1):930. doi: 10.1186/s12889-019-7239-6. BMC Public Health. 2019. PMID: 31296207 Free PMC article.
-
Health Policy Analysis: Applications of Extended Cost-Effectiveness Analysis Methodology in Disease Control Priorities, Third Edition.In: Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, Nugent R, editors. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 27. Chapter 8. In: Jamison DT, Gelband H, Horton S, Jha P, Laxminarayan R, Mock CN, Nugent R, editors. Disease Control Priorities: Improving Health and Reducing Poverty. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 27. Chapter 8. PMID: 30212165 Free Books & Documents. Review.
-
Financial risk protection from out-of-pocket health spending in low- and middle-income countries: a scoping review of the literature.Health Res Policy Syst. 2022 Jul 29;20(1):83. doi: 10.1186/s12961-022-00886-3. Health Res Policy Syst. 2022. PMID: 35906591 Free PMC article.
Cited by
-
Cost of Illness of Epilepsy and Associated Factors in Patients Attending Adult Outpatient Department of University of Gondar Referral Hospital, Northwest Ethiopia.Risk Manag Healthc Policy. 2021 Jun 4;14:2385-2394. doi: 10.2147/RMHP.S289113. eCollection 2021. Risk Manag Healthc Policy. 2021. PMID: 34113193 Free PMC article.
-
A global agenda for older adult immunization in the COVID-19 era: A roadmap for action.Vaccine. 2021 Aug 31;39(37):5240-5250. doi: 10.1016/j.vaccine.2020.06.082. Epub 2020 Jul 3. Vaccine. 2021. PMID: 32703743 Free PMC article.
-
The Lancet NCDI Poverty Commission: bridging a gap in universal health coverage for the poorest billion.Lancet. 2020 Oct 3;396(10256):991-1044. doi: 10.1016/S0140-6736(20)31907-3. Epub 2020 Sep 14. Lancet. 2020. PMID: 32941823 Free PMC article. Review. No abstract available.
-
The burden of household out-of-pocket health expenditures in Ethiopia: estimates from a nationally representative survey (2015-16).Health Policy Plan. 2020 Oct 1;35(8):1003-1010. doi: 10.1093/heapol/czaa044. Health Policy Plan. 2020. PMID: 32772112 Free PMC article.
-
Bending the curve: Modeling the impact of reducing risk factors for noncommunicable diseases to control future health expenditures in Latin America and the Caribbean.PLOS Glob Public Health. 2025 Jul 18;5(7):e0004791. doi: 10.1371/journal.pgph.0004791. eCollection 2025. PLOS Glob Public Health. 2025. PMID: 40680101 Free PMC article.
References
-
- Wagstaff A. Measuring financial protection in health. In: Smith PC, Mossialos E, Papanicolas I, Leatherman S, editors. Performance measurement for health system improvement. Cambridge: Cambridge University Press; 2010.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
