

The modified SAVE score: predicting survival using urgent veno-arterial extracorporeal membrane oxygenation within 24 hours of arrival at the emergency department
- PMID: 27769308
- PMCID: PMC5075192
- DOI: 10.1186/s13054-016-1520-1
The modified SAVE score: predicting survival using urgent veno-arterial extracorporeal membrane oxygenation within 24 hours of arrival at the emergency department
Abstract
Background: Although many risk models have been tested in patients who undergo extracorporeal membrane oxygenation, few have been assessed for patients who received veno-arterial extracorporeal membrane oxygenation (VA-ECMO) support in the emergency department (ED). This study aimed to successfully predict outcomes of patients with cardiac or noncardiac failure who received VA-ECMO in the ED within 24 hours of arrival at the ED.
Method: This retrospective, observational cohort study included 154 patients, who were classified as cardiac (n = 127) and noncardiac (n = 27) patients and received VA-ECMO within 24 hours after arrival at the China Medical University Hospital ED in Taiwan between January 2009 and September 2014. We recorded mechanical ventilation settings, arterial blood gases, laboratory parameters including plasma lactate level, requirement of catecholamines, and risk scores at time of ECMO initiation. ECMO and mechanical ventilation support duration, length of stay in the hospital, and 90-day mortality data were also examined.
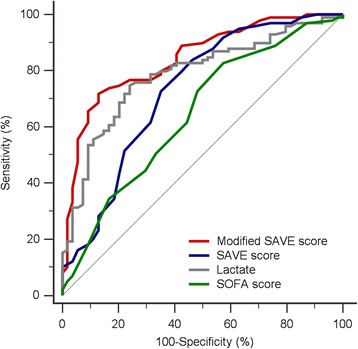
Results: The overall mortality rate was 64.9 %. We used "survival after veno-arterial ECMO (SAVE)" scores to assess survival prediction in survival and nonsurvival groups, which was statistically different (-3.2 vs. -8.3, p <0.001). According to multivariate Cox proportional regression of survival, lactate (hazard ratio [HR] = 1.01, 95 % confidence interval [CI], 1.01-1.01, p <0.001) and SAVE score (HR = 0.92, [95 % CI, 0.88-0.96], p = 0.001) were independent predictors of outcome. Excellent discrimination (area under curve (AUC) = 0.843) was observed when lactate and SAVE score were combined, which we referred to as "the modified SAVE score."
Conclusions: Modified SAVE scores improved outcome prediction for patients who underwent urgent VA-ECMO in the ED.
Keywords: Acute respiratory distress syndrome; Cardiac failure; Critical care; Emergency; Extracorporeal membrane oxygenation; Outcome.
Figures


Comment in
-
Do we need another prognostic score for cardiogenic shock patients with ECMO?Crit Care. 2017 Jul 7;21(1):168. doi: 10.1186/s13054-017-1753-7. Crit Care. 2017. PMID: 28683757 Free PMC article. No abstract available.
References
-
- The Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA. 2011;302:1888–1895. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
