

ESUR recommendations for MR imaging of the sonographically indeterminate adnexal mass: an update
- PMID: 27770228
- PMCID: PMC5408043
- DOI: 10.1007/s00330-016-4600-3
ESUR recommendations for MR imaging of the sonographically indeterminate adnexal mass: an update
Erratum in
-
Erratum to: ESUR recommendations for MR imaging of the sonographically indeterminate adnexal mass: an update.Eur Radiol. 2017 Jun;27(6):2258. doi: 10.1007/s00330-016-4656-0. Eur Radiol. 2017. PMID: 27921156 Free PMC article. No abstract available.
Abstract
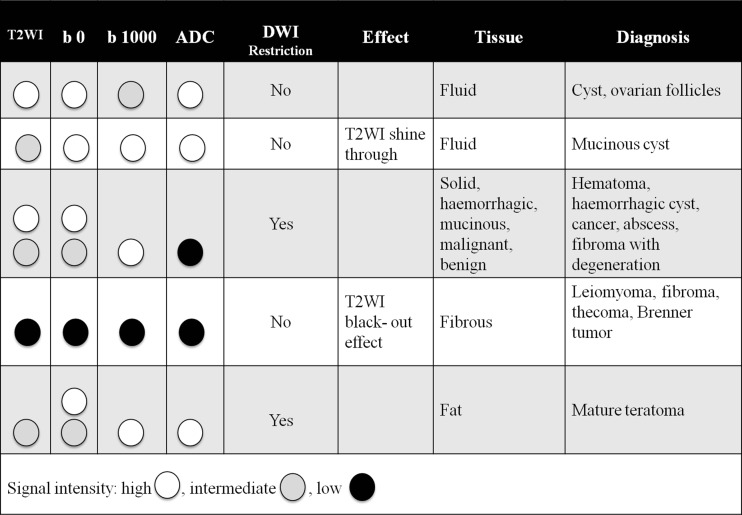
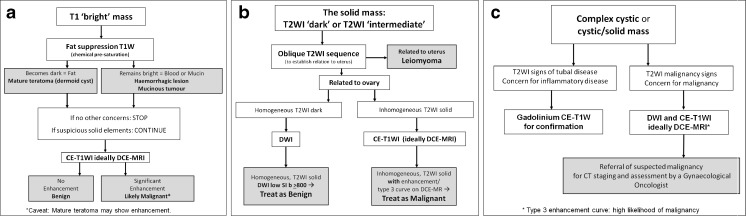
An update of the 2010 published ESUR recommendations of MRI of the sonographically indeterminate adnexal mass integrating functional techniques is provided. An algorithmic approach using sagittal T2 and a set of transaxial T1 and T2WI allows categorization of adnexal masses in one of the following three types according to its predominant signal characteristics. T1 'bright' masses due to fat or blood content can be simply and effectively determined using a combination of T1W, T2W and FST1W imaging. When there is concern for a solid component within such a mass, it requires additional assessment as for a complex cystic or cystic-solid mass. For low T2 solid adnexal masses, DWI is now recommended. Such masses with low DWI signal on high b value image (e.g. > b 1000 s/mm2) can be regarded as benign. Any other solid adnexal mass, displaying intermediate or high DWI signal, requires further assessment by contrast-enhanced (CE)T1W imaging, ideally with DCE MR, where a type 3 curve is highly predictive of malignancy. For complex cystic or cystic-solid masses, both DWI and CET1W-preferably DCE MRI-is recommended. Characteristic enhancement curves of solid components can discriminate between lesions that are highly likely malignant and highly likely benign.
Key points: • MRI is a useful complementary imaging technique for assessing sonographically indeterminate masses. • Categorization allows confident diagnosis in the majority of adnexal masses. • Type 3 contrast enhancement curve is a strong indicator of malignancy. • In sonographically indeterminate masses, complementary MRI assists in triaging patient management.
Keywords: Diagnostic imaging; Magnetic resonance imaging; Ovarian cancer; Ovarian neoplasm; Recommendations.
Figures

References
-
- Spencer JA, Forstner R, Cunha TM, Kinkel K, on behalf of the ESUR Female Imaging Sub-Committee (2010) ESUR guidelines for MR imaging of the sonographically indeterminate adnexal mass: an algorithmic approach. Eur Radiol 20:25–35 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
