

Correction of metabolic acidosis improves insulin resistance in chronic kidney disease
- PMID: 27770799
- PMCID: PMC5075179
- DOI: 10.1186/s12882-016-0372-x
Correction of metabolic acidosis improves insulin resistance in chronic kidney disease
Abstract
Background: Correction of metabolic acidosis (MA) with nutritional therapy or bicarbonate administration is widely used in chronic kidney disease (CKD) patients. However, it is unknown whether these interventions reduce insulin resistance (IR) in diabetic patients with CKD. We sought to evaluate the effect of MA correction on endogenous insulin action in diabetic type 2 (DM2) CKD patients.
Methods: A total of 145 CKD subjects (83 men e 62 women) with DM2 treated with oral antidiabetic drugs were included in the study and followed up to 1 year. All patients were randomly assigned 1:1 to either open-label (A) oral bicarbonate to achieve serum bicarbonate levels of 24-28 mmol/L (treatment group) or (B) no treatment (control group). The Homeostatic model assessment (HOMA) index was used to evaluate IR at study inception and conclusion. Parametric and non-parametric tests as well as linear regression were used.
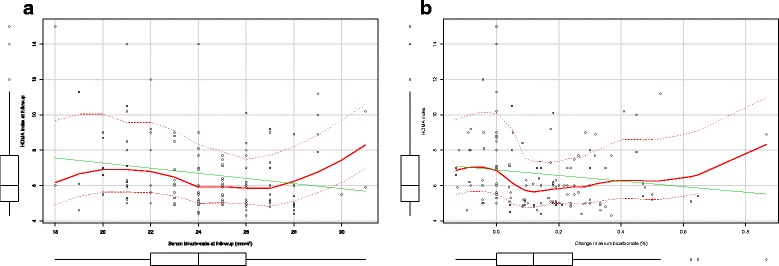
Results: At baseline no differences in demographic and clinical characteristics between the two groups was observed. Average dose of bicarbonate in the treatment group was 0.7 ± 0.2 mmol/kg. Treated patients showed a better metabolic control as confirmed by lower insulin levels (13.4 ± 5.2 vs 19.9 ± 6.3; for treated and control subjects respectively; p < 0.001), Homa-IR (5.9[5.0-7.0] vs 6.3[5.3-8.2]; p = 0.01) and need for oral antidiabetic drugs. The serum bicarbonate and HOMA-IR relationship was non-linear and the largest HOMA-IR reduction was noted for serum bicarbonate levels between 24 and 28 mmol/l. Adjustment for confounders, suggests that serum bicarbonate rather than treatment drives the effect on HOMA-IR.
Conclusions: Serum bicarbonate is related to IR and the largest HOMA-IR reduction is noted for serum bicarbonate between 24 and 28 mmol/l. Treatment with bicarbonate influences IR. However, changes in serum bicarbonate explains the effect of treatment on HOMA index. Future efforts are required to validate these results in diabetic and non-diabetic CKD patients.
Trial registration: The trial was registered at www.clinicaltrial.gov (Use of Bicarbonate in Chronic Renal Insufficiency (UBI) study - NCT01640119 ).
Keywords: CKD; Diabetes; Homa-test; Metabolic acidosis; Sodium bicarbonate.
Figures

References
-
- Collaborators GBDRF, Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, Brauer M, Burnett R, Casey D, Coates MM, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(10010):2287–323. doi: 10.1016/S0140-6736(15)00128-2. - DOI - PMC - PubMed
-
- DALYs GBD, Collaborators H. Murray CJ, Barber RM, Foreman KJ, Abbasoglu Ozgoren A, Abd-Allah F, Abera SF, Aboyans V, Abraham JP, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet. 2015;386(10009):2145–91. doi: 10.1016/S0140-6736(15)61340-X. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
