

Delay in diagnosis of influenza A (H1N1)pdm09 virus infection in critically ill patients and impact on clinical outcome
- PMID: 27770828
- PMCID: PMC5075413
- DOI: 10.1186/s13054-016-1512-1
Delay in diagnosis of influenza A (H1N1)pdm09 virus infection in critically ill patients and impact on clinical outcome
Abstract
Background: Patients infected with influenza A (H1N1)pdm09 virus requiring admission to the ICU remain an important source of mortality during the influenza season. The objective of the study was to assess the impact of a delay in diagnosis of community-acquired influenza A (H1N1)pdm09 virus infection on clinical outcome in critically ill patients admitted to the ICU.
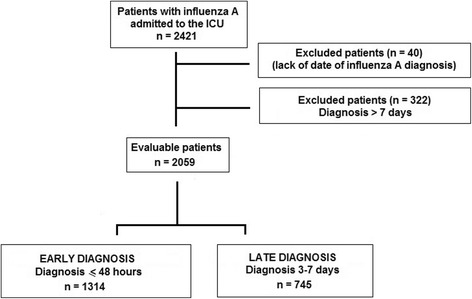
Methods: A prospective multicenter observational cohort study was based on data from the GETGAG/SEMICYUC registry (2009-2015) collected by 148 Spanish ICUs. All patients admitted to the ICU in which diagnosis of influenza A (H1N1)pdm09 virus infection had been established within the first week of hospitalization were included. Patients were classified into two groups according to the time at which the diagnosis was made: early (within the first 2 days of hospital admission) and late (between the 3rd and 7th day of hospital admission). Factors associated with a delay in diagnosis were assessed by logistic regression analysis.
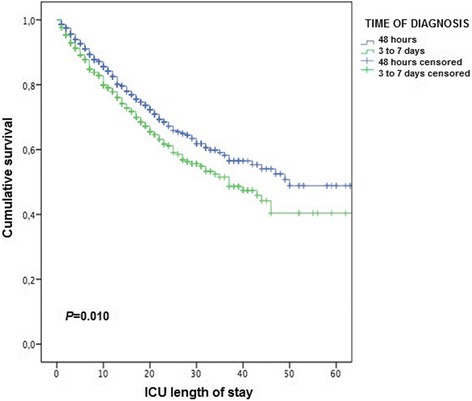
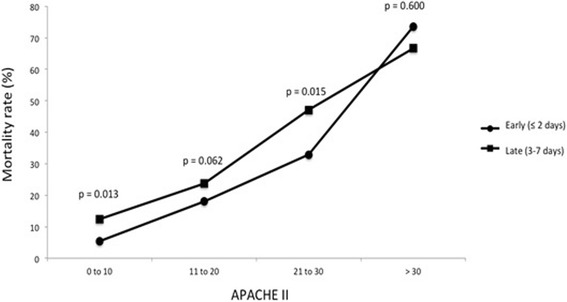
Results: In 2059 ICU patients diagnosed with influenza A (H1N1)pdm09 virus infection within the first 7 days of hospitalization, the diagnosis was established early in 1314 (63.8 %) patients and late in the remaining 745 (36.2 %). Independent variables related to a late diagnosis were: age (odds ratio (OR) = 1.02, 95 % confidence interval (CI) 1.01-1.03, P < 0.001); first seasonal period (2009-2012) (OR = 2.08, 95 % CI 1.64-2.63, P < 0.001); days of hospital stay before ICU admission (OR = 1.26, 95 % CI 1.17-1.35, P < 0.001); mechanical ventilation (OR = 1.58, 95 % CI 1.17-2.13, P = 0.002); and continuous venovenous hemofiltration (OR = 1.54, 95 % CI 1.08-2.18, P = 0.016). The intra-ICU mortality was significantly higher among patients with late diagnosis as compared with early diagnosis (26.9 % vs 17.1 %, P < 0.001). Diagnostic delay was one independent risk factor for mortality (OR = 1.36, 95 % CI 1.03-1.81, P < 0.001).
Conclusions: Late diagnosis of community-acquired influenza A (H1N1)pdm09 virus infection is associated with a delay in ICU admission, greater possibilities of respiratory and renal failure, and higher mortality rate. Delay in diagnosis of flu is an independent variable related to death.
Keywords: Critically ill; Early diagnosis; ICU; Influenza A (H1N1)pdm09 virus infection; Late diagnosis; Mortality; Outcome.
Figures
References
-
- Streng A, Prifert C, Weissbrich B, Liese JG, Bavarian PICU Study Group on Influenza and Other Viral ARI Continued high incidence of children with severe influenza A(H1N1)pdm09 admitted to paediatric intensive care units in Germany during the first three post-pandemic influenza seasons, 2010/11-2012/13. BMC Infect Dis. 2015;15:573. doi: 10.1186/s12879-015-1293-1. - DOI - PMC - PubMed
-
- Puskarich MA, Trzeciak S, Shapiro NI, Arnold RC, Horton JM, Studnek JR, Emergency Medicine Shock Research Network (EMSHOCKNET) et al. Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol. Crit Care Med. 2011;39:2066–71. doi: 10.1097/CCM.0b013e31821e87ab. - DOI - PMC - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637. doi: 10.1097/CCM.0b013e31827e83af. - DOI - PubMed
-
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42:1749–55. doi: 10.1097/CCM.0000000000000330. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
