

Ventricular conduction abnormalities as predictors of long-term survival in acute de novo and decompensated chronic heart failure
- PMID: 27774265
- PMCID: PMC5061091
- DOI: 10.1002/ehf2.12068
Ventricular conduction abnormalities as predictors of long-term survival in acute de novo and decompensated chronic heart failure
Abstract
Aims: Data on the prognostic role of left and right bundle branch blocks (LBBB and RBBB), and nonspecific intraventricular conduction delay (IVCD; QRS ≥ 110 ms, no BBB) in acute heart failure (AHF) are controversial. Our aim was to investigate electrocardiographic predictors of long-term survival in patients with de novo AHF and acutely decompensated chronic heart failure (ADCHF).
Methods and results: We analysed the admission electrocardiogram of 982 patients from a multicenter European cohort of AHF with 3.9 years' mean follow-up. Half (51.5%, n = 506) of the patients had de novo AHF. LBBB, and IVCD were more common in ADCHF than in de novo AHF: 17.2% vs. 8.7% (P < 0.001) and 20.6% vs. 13.2% (P = 0.001), respectively, and RBBB was almost equally common (6.9% and 8.1%; P = 0.5), respectively. Mortality during the follow-up was higher in patients with RBBB (85.4%) and IVCD (73.7%) compared with patients with normal ventricular conduction (57.0%); P < 0.001 for both. The impact of RBBB on prognosis was prominent in de novo AHF (adjusted HR 1.93, 1.03-3.60; P = 0.04), and IVCD independently predicted death in ADCHF (adjusted HR 1.79, 1.28-2.52; P = 0.001). Both findings were pronounced in patients with reduced ejection fraction. LBBB showed no association with increased mortality in either of the subgroups. The main results were confirmed in a validation cohort of 1511 AHF patients with 5.9 years' mean follow-up.
Conclusions: Conduction abnormalities predict long-term survival differently in de novo AHF and ADCHF. RBBB predicts mortality in de novo AHF, and IVCD in ADCHF. LBBB has no additive predictive value in AHF requiring hospitalization.
Keywords: Acute heart failure; Bundle branch block; Prognosis; Ventricular conduction; de novo.
Figures
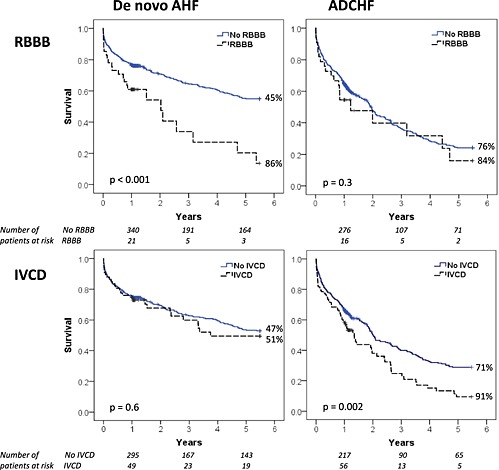

 for each type of conduction abnormality in all patients (solid lines) and in the subgroups of de novo AHF and ADCHF (dashed lines) in the derivation cohort.
for each type of conduction abnormality in all patients (solid lines) and in the subgroups of de novo AHF and ADCHF (dashed lines) in the derivation cohort.Similar articles
-
The prognostic significance of bundle branch block in acute heart failure: a systematic review and meta-analysis.Clin Res Cardiol. 2023 Aug;112(8):1020-1043. doi: 10.1007/s00392-022-02105-z. Epub 2022 Sep 18. Clin Res Cardiol. 2023. PMID: 36116092
-
Long-term survival after hospitalization for acute heart failure--differences in prognosis of acutely decompensated chronic and new-onset acute heart failure.Int J Cardiol. 2013 Sep 20;168(1):458-62. doi: 10.1016/j.ijcard.2012.09.128. Epub 2012 Oct 13. Int J Cardiol. 2013. PMID: 23073273
-
Upgrade and de novo cardiac resynchronization therapy: impact of paced or intrinsic QRS morphology on outcomes and survival.Heart Rhythm. 2009 Oct;6(10):1439-47. doi: 10.1016/j.hrthm.2009.07.009. Epub 2009 Jul 10. Heart Rhythm. 2009. PMID: 19717348
-
Differences in Mortality of New-Onset (De-Novo) Acute Heart Failure Versus Acute Decompensated Chronic Heart Failure.Am J Cardiol. 2019 Aug 15;124(4):554-559. doi: 10.1016/j.amjcard.2019.05.031. Epub 2019 May 25. Am J Cardiol. 2019. PMID: 31221464
-
Differences in clinical characteristics and outcome of de novo heart failure compared to acutely decompensated chronic heart failure - systematic review and meta-analysis.Acta Cardiol. 2021 Jun;76(4):410-420. doi: 10.1080/00015385.2020.1747178. Epub 2020 Apr 7. Acta Cardiol. 2021. PMID: 32252602
Cited by
-
Ventricular Conduction Disturbance in Acute Heart Failure Syndrome: Does It Matter for Prognosis?Korean Circ J. 2019 Jul;49(7):612-614. doi: 10.4070/kcj.2019.0116. Epub 2019 May 2. Korean Circ J. 2019. PMID: 31165596 Free PMC article. No abstract available.
-
Prognostic Implication of Ventricular Conduction Disturbance Pattern in Hospitalized Patients with Acute Heart Failure Syndrome.Korean Circ J. 2019 Jul;49(7):602-611. doi: 10.4070/kcj.2018.0290. Epub 2019 Feb 26. Korean Circ J. 2019. PMID: 30891964 Free PMC article.
-
Obesity and Cardiac Conduction Block Disease in China.JAMA Netw Open. 2023 Nov 1;6(11):e2342831. doi: 10.1001/jamanetworkopen.2023.42831. JAMA Netw Open. 2023. PMID: 37955899 Free PMC article.
-
The prognostic significance of bundle branch block in acute heart failure: a systematic review and meta-analysis.Clin Res Cardiol. 2023 Aug;112(8):1020-1043. doi: 10.1007/s00392-022-02105-z. Epub 2022 Sep 18. Clin Res Cardiol. 2023. PMID: 36116092
-
Age-Stratified Clinical Outcome in Patients with Known Heart Failure Who Receive Pacemaker, Resynchronization Therapy, or Defibrillator Implants.Cardiology. 2024;149(5):474-483. doi: 10.1159/000538529. Epub 2024 Mar 30. Cardiology. 2024. PMID: 38555639 Free PMC article.
References
-
- Kashani A, Barold SS. Significance of QRS complex duration in patients with heart failure. J Am Coll Cardiol 2005; 46: 2183–92. - PubMed
-
- Wang NC, Maggioni AP, Konstam MA, Zannad F, Krasa HB, Burnett JC Jr, Grinfeld L, Swedberg K, Udelson JE, Cook T, Traver B, Zimmer C, Orlandi C, Gheorghiade M. Efficacy of vasopressin antagonism in heart failure outcome study with tolvaptan I. Clinical implications of QRS duration in patients hospitalized with worsening heart failure and reduced left ventricular ejection fraction. JAMA 2008; 299: 2656–66. - PubMed
-
- Mueller C, Laule‐Kilian K, Klima T, Breidthardt T, Hochholzer W, Perruchoud AP, Christ M. Right bundle branch block and long‐term mortality in patients with acute congestive heart failure. J Intern Med 2006; 260: 421–8. - PubMed
-
- Huvelle E, Fay R, Alla F, Cohen Solal A, Mebazaa A, Zannad F. Left bundle branch block and mortality in patients with acute heart failure syndrome: a substudy of the EFICA cohort. Eur J Heart Fail 2010; 12(2): 156–63. - PubMed
-
- Barsheshet A, Goldenberg I, Garty M, Gottlieb S, Sandach A, Laish‐Farkash A, Eldar M, Glikson M. Relation of bundle branch block to long‐term (four‐year) mortality in hospitalized patients with systolic heart failure. Am J Cardiol 2011; 107: 540–4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
