

Impact of Cervical Dystonia on Work Productivity: An Analysis From a Patient Registry
- PMID: 27774495
- PMCID: PMC5064605
- DOI: 10.1002/mdc3.12238
Impact of Cervical Dystonia on Work Productivity: An Analysis From a Patient Registry
Abstract
Background: Cervical dystonia is thought to result in high disease burden, but limited information exists on its impact on employment and work productivity. We utilized data from the Cervical Dystonia Patient Registry for the Observation of OnabotulinumtoxinA Efficacy (ClinicalTrials.gov identifier: NCT00836017) to assess the impact of cervical dystonia on employment and work productivity and examine the effect of onabotulinumtoxinA treatments on work productivity.
Methods: Subjects completed a questionnaire on employment status and work productivity at baseline and final visit. Baseline data were examined by severity of cervical dystonia, predominant subtype, presence of pain, prior exposure to botulinum toxin, and/or utility of a sensory trick. Work productivity results at baseline and final visit were compared in subjects who were toxin-naïve at baseline and received three onabotulinumtoxinA treatments.
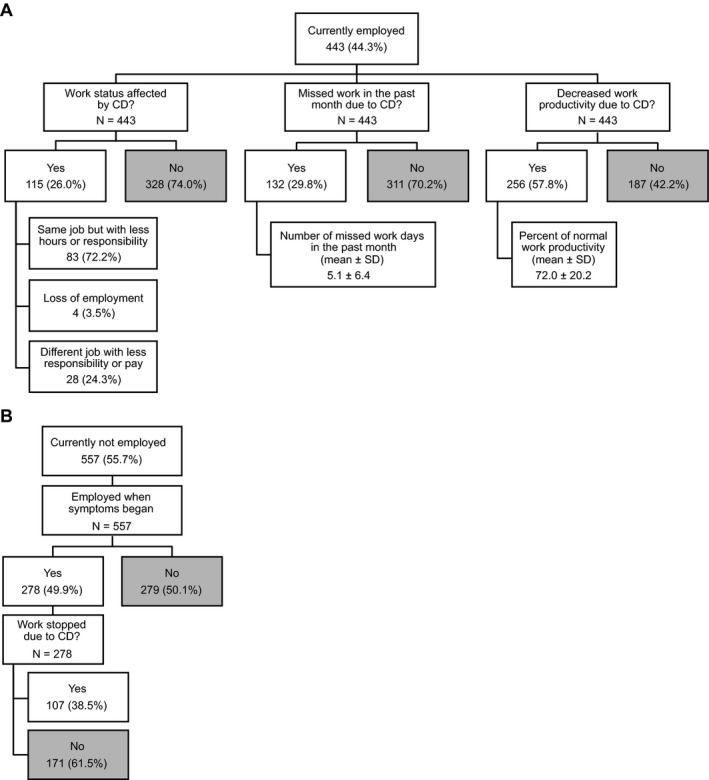
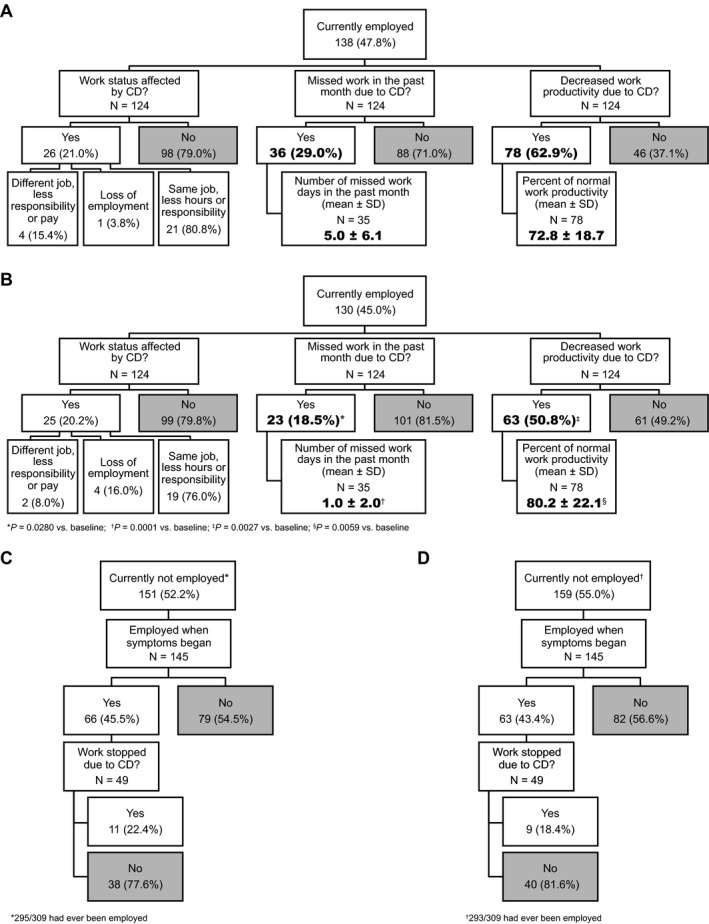
Results: Of 1,038 subjects, 42.8% were employed full- or part-time, 6.1% unemployed, 32.7% retired, and 11.8% disabled. Of those currently employed, cervical dystonia affected work status of 26.0%, caused 29.8% to miss work in the past month (mean, 5.1 ± 6.4 days), and 57.8% reported decreased productivity. Half of those unemployed were employed when symptoms began, and 38.5% attributed lost employment to cervical dystonia. Pain, increasing severity, and anterocollis/retrocollis had the largest effects on work status/productivity. Preliminary analyses showed that absenteeism and presenteeism were significantly decreased following onabotulinumtoxinA treatments in the subpopulation that was toxin-naïve at baseline.
Conclusions: This analysis confirms the substantial negative impact of cervical dystonia on employment, with cervical dystonia-associated pain being a particularly important driver. OnabotulinumtoxinA treatment appears to improve work productivity.
Keywords: botulinum toxin; cervical dystonia; employment.
Figures
Similar articles
-
Neck Pain and Cervical Dystonia: Treatment Outcomes from CD PROBE (Cervical Dystonia Patient Registry for Observation of OnabotulinumtoxinA Efficacy).Pain Pract. 2016 Nov;16(8):1073-1082. doi: 10.1111/papr.12408. Epub 2016 Feb 23. Pain Pract. 2016. PMID: 26910788
-
Concurrent onabotulinumtoxinA treatment of cervical dystonia and concomitant migraine.Headache. 2012 Sep;52(8):1219-25. doi: 10.1111/j.1526-4610.2012.02164.x. Epub 2012 May 18. Headache. 2012. PMID: 22607530 Clinical Trial.
-
Primary results from the cervical dystonia patient registry for observation of onabotulinumtoxina efficacy (CD PROBE).J Neurol Sci. 2015 Feb 15;349(1-2):84-93. doi: 10.1016/j.jns.2014.12.030. Epub 2014 Dec 27. J Neurol Sci. 2015. PMID: 25595221 Clinical Trial.
-
Patient considerations in the treatment of cervical dystonia: focus on botulinum toxin type A.Patient Prefer Adherence. 2015 Jun 2;9:725-31. doi: 10.2147/PPA.S75459. eCollection 2015. Patient Prefer Adherence. 2015. PMID: 26082621 Free PMC article. Review.
-
Botulinum toxin B: a review of its therapeutic potential in the management of cervical dystonia.Drugs. 2002;62(4):705-22. doi: 10.2165/00003495-200262040-00011. Drugs. 2002. PMID: 11893235 Review.
Cited by
-
Abnormal regional homogeneity and its relationship with symptom severity in cervical dystonia: a rest state fMRI study.BMC Neurol. 2021 Feb 5;21(1):55. doi: 10.1186/s12883-021-02079-x. BMC Neurol. 2021. PMID: 33546628 Free PMC article.
-
Job preservation by an office worker with idiopathic cervical dystonia: case report.Med Lav. 2020 Aug 26;111(6):457-462. doi: 10.23749/mdl.v111i6.9874. Med Lav. 2020. PMID: 33311421 Free PMC article.
-
It's tricky: Rating alleviating maneuvers in cervical dystonia.J Neurol Sci. 2020 Dec 15;419:117205. doi: 10.1016/j.jns.2020.117205. Epub 2020 Nov 1. J Neurol Sci. 2020. PMID: 33160248 Free PMC article.
-
Sensory Tricks Are Associated with Higher Sleep-Related Quality of Life in Cervical Dystonia.Tremor Other Hyperkinet Mov (N Y). 2019 Jun 17;9. doi: 10.7916/4q53-vt23. eCollection 2019. Tremor Other Hyperkinet Mov (N Y). 2019. PMID: 31413893 Free PMC article.
-
Comorbidity and retirement in cervical dystonia.J Neurol. 2019 Sep;266(9):2216-2223. doi: 10.1007/s00415-019-09402-0. Epub 2019 May 31. J Neurol. 2019. PMID: 31152297 Free PMC article.
References
-
- Chan J, Brin MF, Fahn S. Idiopathic cervical dystonia: clinical characteristics. Mov Disord 1991;6:119–126. - PubMed
-
- Phukan J, Albanese A, Gasser T, Warner T. Primary dystonia and dystonia‐plus syndromes: clinical characteristics, diagnosis, and pathogenesis. Lancet Neurol 2011;10:1074–1085. - PubMed
-
- Rondot P, Marchand MP, Dellatolas G. Spasmodic torticollis—review of 220 patients. Can J Neurol Sci 1991;18:143–151. - PubMed
-
- Molho ES, Feustel PJ, Factor SA. Clinical comparison of tardive and idiopathic cervical dystonia. Mov Disord 1998;13:486–489. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
