

A Novel Model of Transient Occlusion of the Middle Cerebral Artery in Awake Mice
- PMID: 27774515
- PMCID: PMC5074053
A Novel Model of Transient Occlusion of the Middle Cerebral Artery in Awake Mice
Abstract
Background: Stroke is one of the leading causes of death and disability worldwide. As a consequence, several excellent rodent models have been developed to gain insight into the pathophysiology of stroke and testing the efficacy of neuroprotective interventions. However, one potential problem is that albeit roughly 80% of strokes occur in awake patients, all existing murine stroke models employ anesthesia. Moreover, epidemiological studies have shown that stroke injury is more severe in the minority of patients that suffer stroke while asleep. To better mimic the clinical situation, it is therefore preferable to analyze the pathobiology of experimental stroke in awake animals.
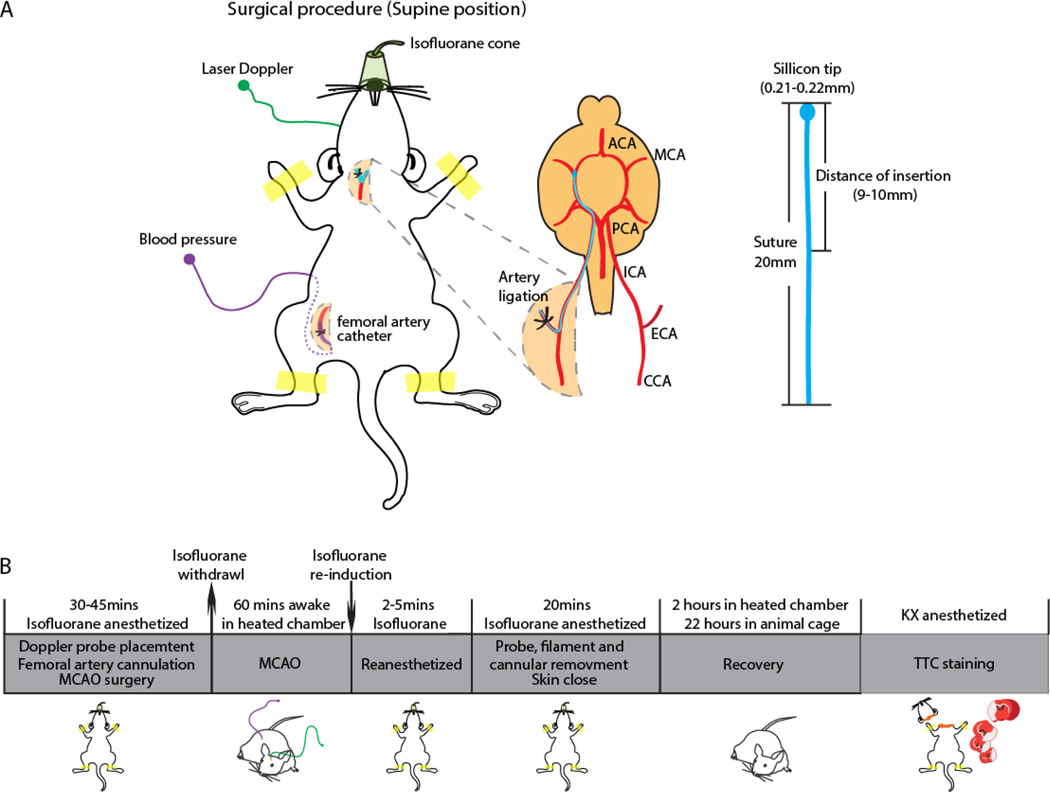
New method: This model of transient middle cerebral artery occlusion (MCAO) in awake mice is based on insertion of an intraluminal suture via the external carotid artery during isoflurane anesthesia. Isoflurane is discontinued during the 60 min MCAO while cerebral blood flow is continuously monitored using laser doppler in the awake unrestrained mouse.
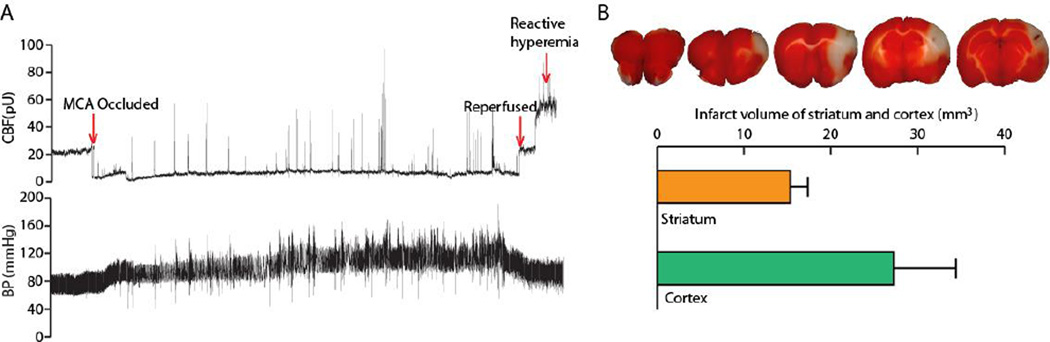
Results: Sixty minutes of awake MCAO model reliably induced infarction in striatum and cortex (relative infarct volume is 24.34% of contralateral hemisphere volume; absolute infarct volume is 47.94 mm3).
Comparison with existing methods: The animals in this method are awake during the one hour occlusion period, which may provide a more translational research approach than existing methods that apply anesthesia during the occlusion.
Conclusions: Since the state of brain activity likely affects stroke injury and most anesthetics have neuroprotective effects, this model more accurately mimics the condition during which the majority of human ischemic stroke occurs.
Keywords: Awake Mouse; MCAO; Stroke; Transient MCAO.
Figures
References
-
- Brott T, Bogousslavsky J. Treatment of acute ischemic stroke. The New England journal of medicine. 2000;343:710–722. - PubMed
-
- Busto R, Dietrich WD, Globus MY, Valdes I, Scheinberg P, Ginsberg MD. Small differences in intraischemic brain temperature critically determine the extent of ischemic neuronal injury. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 1987;7:729–738. - PubMed
-
- Campbell BCV, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, Yan B, Dowling RJ, Parsons MW, Oxley TJ, Wu TY, Brooks M, Simpson MA, Miteff F, Levi CR, Krause M, Harrington TJ, Faulder KC, Steinfort BS, Priglinger M, Ang T, Scroop R, Barber PA, McGuinness B, Wijeratne T, Phan TG, Chong W, Chandra RV, Bladin CF, Badve M, Rice H, de Villiers L, Ma H, Desmond PM, Donnan GA, Davis SM Investigators E-I. Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection. New Engl J Med. 2015;372:1009–1018. - PubMed
-
- Chaturvedi S, Adams HP, Jr, Woolson RF. Circadian variation in ischemic stroke subtypes. Stroke; a journal of cerebral circulation. 1999;30:1792–1795. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials