

A Comparison of the Effects of Continuous versus Discontinuous Movement Patterns on Parkinsonian Rigidity and Reflex Responses to Passive Stretch and Shortening
- PMID: 27774516
- PMCID: PMC5070564
A Comparison of the Effects of Continuous versus Discontinuous Movement Patterns on Parkinsonian Rigidity and Reflex Responses to Passive Stretch and Shortening
Abstract
Objective: Quantify the effect of a continuous compared to discontinuous movement trajectory on parkinsonian rigidity and reflex responses to passive stretch and shortening.
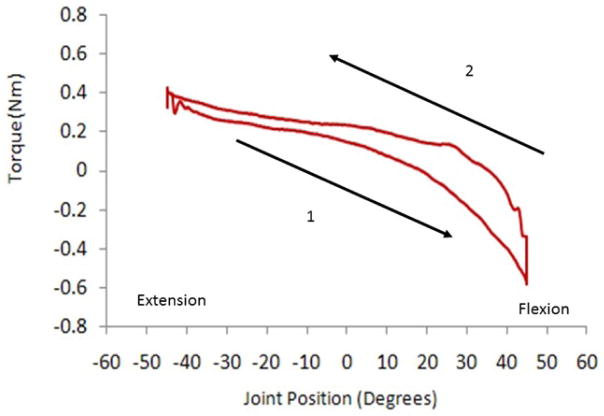
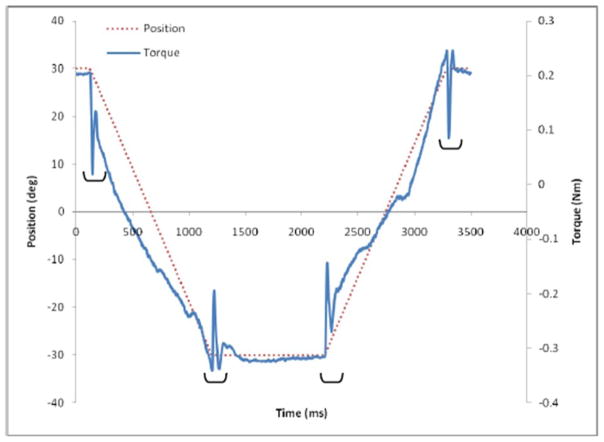
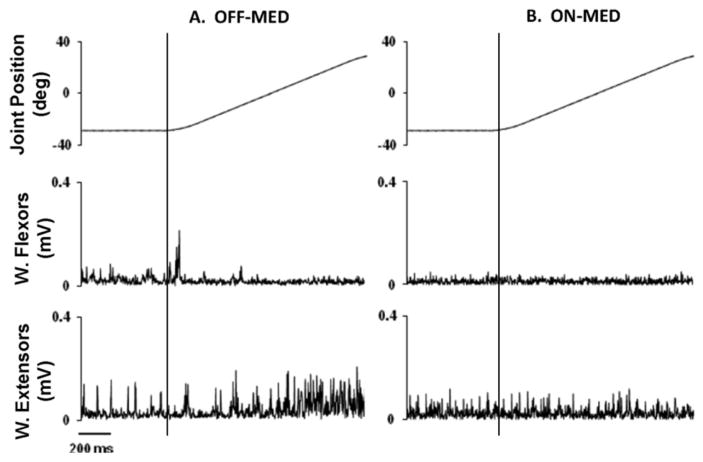
Methods: Eighteen participants with Parkinson's disease (PD) performed passive wrist flexion and extension movements through a 90° range of motion at 50 °/sec using continuous (CONT) and discontinuous (DISC) movement trajectories. Participants were tested in both the OFF-MED and ON-MED states. Rigidity was quantified by rigidity work score and slopes of the moment-angle plots during both flexion and extension. Reflex response was quantified by mean EMG amplitudes of forearm musculature.
Results: No differences were observed between CONT and DISC for rigidity (p = 0.18) or moment-angle plot slopes (Flexion: p = 0.97; Extension: p = 0.89). However, medication was associated with reductions in rigidity (p = 0.02) and increases in moment-angle plot slopes (Flexion: p = 0.03; Extension: p = 0.02). The CONT compared to DISC trajectory was associated with greater EMG amplitudes in the shortened muscles (p = 0.04) and smaller EMG ratios (p < 0.05) during flexion, and greater EMG amplitudes in the lengthened muscles (p = 0.02) during extension. Dopaminergic medication reduced EMG amplitudes in stretched muscles during extension (p < 0.05).
Conclusions: The nature of the movement trajectory (continuous vs. discontinuous) used during clinical assessment does not alter the presentation of rigidity in PD. Rigidity is reduced with the administration of dopaminergic medication, independent of movement trajectory.
Significance: These data suggest that the presentation of rigidity used in the determination of diagnosis, treatment and prognosis in PD will not be affected by the continuous nature of the movement trajectory used during clinical assessment.
Keywords: Dopaminergic medication; EMG; Kinetics; Parkinson’s disease; Rigidity.
Conflict of interest statement
No conflicts declared.
Figures
References
-
- Andrews CJ, Burke D, Lance JW. The response to muscle stretch and shortening in Parkinsonian rigidity. Brain. 1972;95:795–812. - PubMed
-
- Angel RW. Muscular contractions elicited by passive shortening. Adv Neurol. 1983;39:555–563. - PubMed
-
- Berardelli A, Hallett M. Shortening reaction of human tibialis anterior. Neurology. 1984;34:242–245. - PubMed
-
- Bergui M, Lopiano L, Paglia G, Quattrocolo G, Scarzella L, Bergamasco B. Stretch reflex of quadriceps femoris and its relation to rigidity in Parkinson’s disease. Acta Neurol Scand. 1992;86:226–229. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous