

The Estimated Verbal GCS Subscore in Intubated Traumatic Brain Injury Patients: Is it Really Better?
- PMID: 27774844
- PMCID: PMC5397225
- DOI: 10.1089/neu.2016.4657
The Estimated Verbal GCS Subscore in Intubated Traumatic Brain Injury Patients: Is it Really Better?
Abstract
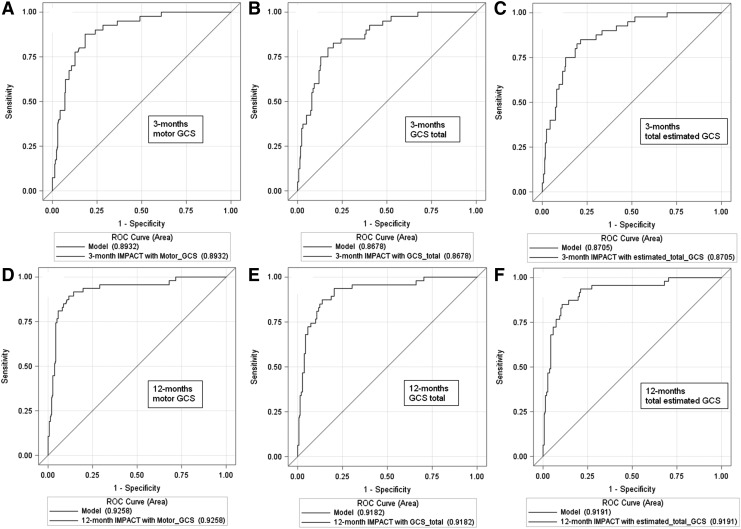
The Glasgow Coma Scale (GCS) has limited utility in intubated patients due to the inability to assign verbal subscores. The verbal subscore can be derived from the eye and motor subscores using a mathematical model, but the advantage of this method and its use in outcome prognostication in traumatic brain injury (TBI) patients remains unknown. We compared the validated "Core+CT"-IMPACT-model performance in 251 intubated TBI patients prospectively enrolled in the longitudinal OPTIMISM study between November 2009 and May 2015 when substituting the original motor GCS (mGCS) with the total estimated GCS (teGCS; with estimated verbal subscore). We hypothesized that model performance would improve with teGCS. Glasgow Outcome Scale (GOS) scores were assessed at 3 and 12 months by trained interviewers. In the complete case analysis, there was no statistically or clinically significant difference in the discrimination (C-statistic) at either time-point using the mGCS versus the teGCS (3 months: 0.893 vs. 0.871;12 months: 0.926 vs. 0.92). At 3 months, IMPACT-model calibration was excellent with mGCS and teGCS (Hosmer-Lemeshow "goodness-of-fit" chi square p value 0.9293 and 0.9934, respectively); it was adequate at 12 months with teGCS (0.5893) but low with mGCS (0.0158), possibly related to diminished power at 12 months. At both time-points, motor GCS contributed more to the variability of outcome (Nagelkerke ΔR2) than teGCS (3 months: 5.8% vs. 0.4%; 12 months: 5% vs. 2.6%). The sensitivity analysis with imputed missing outcomes yielded similar results, with improved calibration for both GCS variants. In our cohort of intubated TBI patients, there was no statistically or clinically meaningful improvement in the IMPACT-model performance by substituting the original mGCS with teGCS.
Keywords: Glasgow Coma Scale; estimated verbal GCS; motor GCS; outcome prognostication; traumatic brain injury.
Conflict of interest statement
No competing financial interests exist.
Figures

Similar articles
-
A comparison of the prehospital motor component of the Glasgow coma scale (mGCS) to the prehospital total GCS (tGCS) as a prehospital risk adjustment measure for trauma patients.Prehosp Emerg Care. 2014 Jan-Mar;18(1):68-75. doi: 10.3109/10903127.2013.844870. Prehosp Emerg Care. 2014. PMID: 24329032
-
Simplifying the use of prognostic information in traumatic brain injury. Part 1: The GCS-Pupils score: an extended index of clinical severity.J Neurosurg. 2018 Jun;128(6):1612-1620. doi: 10.3171/2017.12.JNS172780. Epub 2018 Apr 10. J Neurosurg. 2018. PMID: 29631516
-
Simplifying the use of prognostic information in traumatic brain injury. Part 2: Graphical presentation of probabilities.J Neurosurg. 2018 Jun;128(6):1621-1634. doi: 10.3171/2017.12.JNS172782. Epub 2018 Apr 10. J Neurosurg. 2018. PMID: 29631517
-
The Predictive Value of the Verbal Glasgow Coma Scale in Traumatic Brain Injury: A Systematic Review.J Head Trauma Rehabil. 2024 Jul-Aug 01;39(4):273-283. doi: 10.1097/HTR.0000000000000938. Epub 2024 Feb 27. J Head Trauma Rehabil. 2024. PMID: 38453630
-
[Glasgow Coma Scale in traumatic brain injury].Anaesthesist. 2004 Dec;53(12):1245-55; quiz 1256. doi: 10.1007/s00101-004-0777-y. Anaesthesist. 2004. PMID: 15597166 Review. German.
Cited by
-
Impact of Acid-Base Status on Mortality in Patients with Acute Pesticide Poisoning.Toxics. 2021 Jan 23;9(2):22. doi: 10.3390/toxics9020022. Toxics. 2021. PMID: 33498605 Free PMC article.
-
Machine learning predictors of risk of death within 7 days in patients with non-traumatic subarachnoid hemorrhage in the intensive care unit: A multicenter retrospective study.Heliyon. 2023 Dec 16;10(1):e23943. doi: 10.1016/j.heliyon.2023.e23943. eCollection 2024 Jan 15. Heliyon. 2023. PMID: 38192749 Free PMC article.
-
Machine Learning Reveals Demographic Disparities in Palliative Care Timing Among Patients With Traumatic Brain Injury Receiving Neurosurgical Consultation.Neurocrit Care. 2025 Jun;42(3):953-964. doi: 10.1007/s12028-024-02172-2. Epub 2024 Dec 10. Neurocrit Care. 2025. PMID: 39653977
-
Comparison of full outline of unresponsiveness score and Glasgow Coma Scale in Medical Intensive Care Unit.Ann Card Anaesth. 2019 Apr-Jun;22(2):143-148. doi: 10.4103/aca.ACA_25_18. Ann Card Anaesth. 2019. PMID: 30971594 Free PMC article.
-
Prediction of Mortality in the Medical Intensive Care Unit with Serial Full Outline of Unresponsiveness Score in Elderly Patients.Indian J Crit Care Med. 2022 Jan;26(1):94-99. doi: 10.5005/jp-journals-10071-24094. Indian J Crit Care Med. 2022. PMID: 35110851 Free PMC article.
References
-
- Teasdale G., and Jennett B. (1974). Assessment of coma and impaired consciousness. A practical scale. Lancet 2, 81–84 - PubMed
-
- Champion H.R., Copes W.S., Sacco W.J., Lawnick M.M., Keast S.L., Bain L.W., Jr., Flanagan M.E., and Frey C.F. (1990). The Major Trauma Outcome Study: establishing national norms for trauma care. J. Trauma 30, 1356–1365 - PubMed
-
- Champion H.R., Sacco W.J., Carnazzo A.J., Copes W., and Fouty W.J. (1981). Trauma score. Crit. Care Med. 9, 672–676 - PubMed
-
- Niskanen M., Kari A., Nikki P., Iisalo E., Kaukinen L., Rauhala V., Saarela E., and Halinen M. (1991). Acute physiology and chronic health evaluation (APACHE II) and Glasgow coma scores as predictors of outcome from intensive care after cardiac arrest. Crit. Care Med. 19, 1465–1473 - PubMed
-
- Steyerberg E.W., Mushkudiani N., Perel P., Butcher I., Lu J., McHugh G.S., Murray G.D., Marmarou A., Roberts I., Habbema J.D., and Maas A.I. (2008). Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS Med. 5, e165. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
