

Basal Tumor Cell Isolation and Patient-Derived Xenograft Engraftment Identify High-Risk Clinical Bladder Cancers
- PMID: 27775025
- PMCID: PMC5075783
- DOI: 10.1038/srep35854
Basal Tumor Cell Isolation and Patient-Derived Xenograft Engraftment Identify High-Risk Clinical Bladder Cancers
Abstract
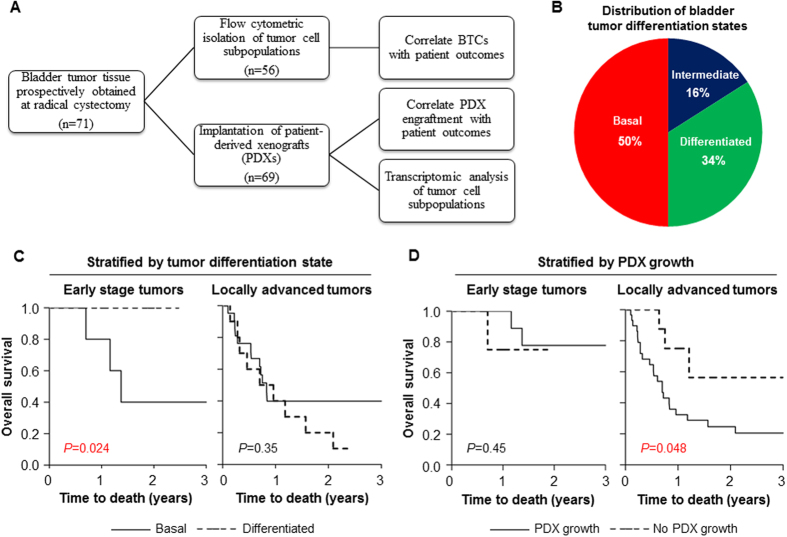
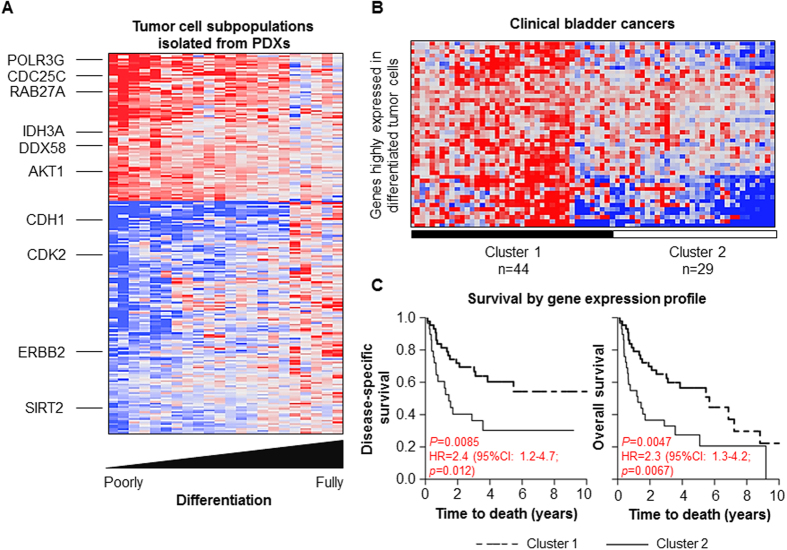
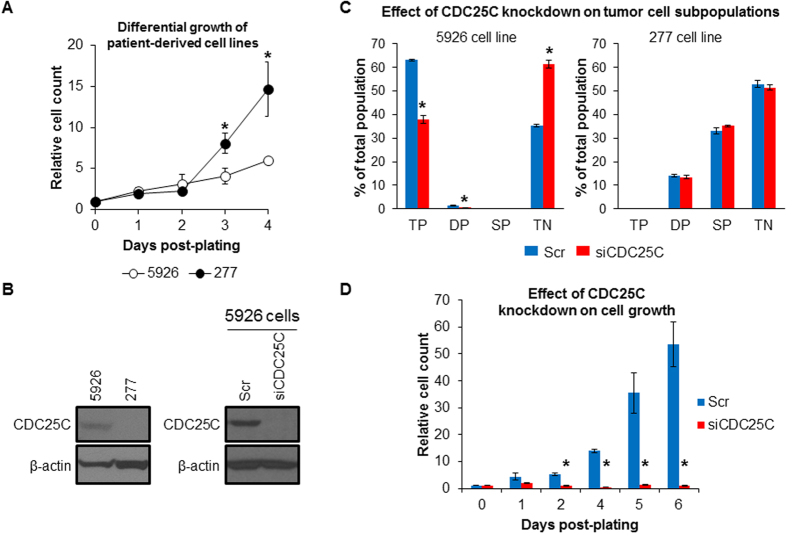
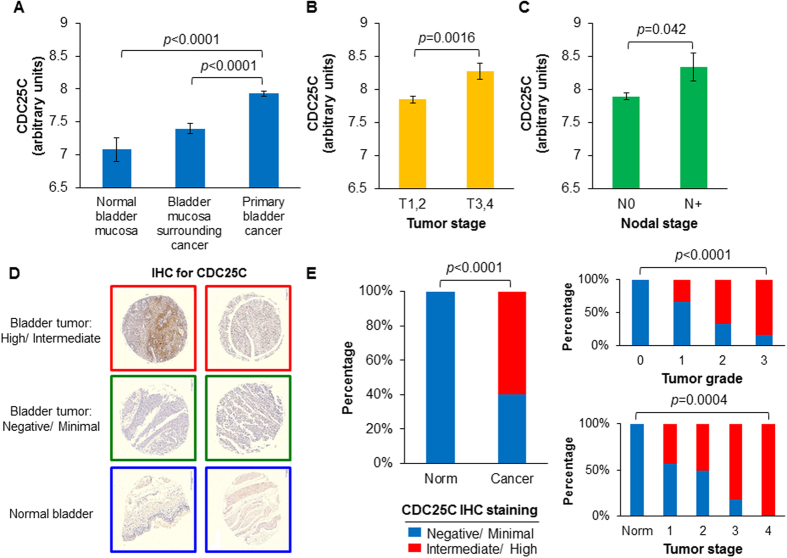
Strategies to identify tumors at highest risk for treatment failure are currently under investigation for patients with bladder cancer. We demonstrate that flow cytometric detection of poorly differentiated basal tumor cells (BTCs), as defined by the co-expression of CD90, CD44 and CD49f, directly from patients with early stage tumors (T1-T2 and N0) and patient-derived xenograft (PDX) engraftment in locally advanced tumors (T3-T4 or N+) predict poor prognosis in patients with bladder cancer. Comparative transcriptomic analysis of bladder tumor cells isolated from PDXs indicates unique patterns of gene expression during bladder tumor cell differentiation. We found cell division cycle 25C (CDC25C) overexpression in poorly differentiated BTCs and determined that CDC25C expression predicts adverse survival independent of standard clinical and pathologic features in bladder cancer patients. Taken together, our findings support the utility of BTCs and bladder cancer PDX models in the discovery of novel molecular targets and predictive biomarkers for personalizing oncology care for patients.
Figures
References
-
- Siegel R. L., Miller K. D. & Jemal A.. Cancer statistics, 2016: Cancer Statistics, 2016. CA. Cancer J. Clin. 66, 7–30 (2016). - PubMed
-
- Shah J. B., McConkey D. J. & Dinney C. P. N.. New strategies in muscle-invasive bladder cancer: on the road to personalized medicine. Clin. Cancer Res. 17, 2608–2612 (2011). - PubMed
-
- Advanced Bladder Cancer (ABC) Meta-analysis Collaboration. Neoadjuvant chemotherapy in invasive bladder cancer: update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur. Urol. 48, 202–205; discussion 205–206 (2005). - PubMed
-
- Grossman H. B. et al.. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N. Engl. J. Med. 349, 859–866 (2003). - PubMed
-
- Galsky M. D. et al.. Effectiveness of Adjuvant Chemotherapy for Locally Advanced Bladder Cancer. J. Clin. Oncol. 34, 825–832 (2016). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
