

Multiplatform-based molecular subtypes of non-small-cell lung cancer
- PMID: 27775076
- PMCID: PMC5344748
- DOI: 10.1038/onc.2016.303
Multiplatform-based molecular subtypes of non-small-cell lung cancer
Abstract
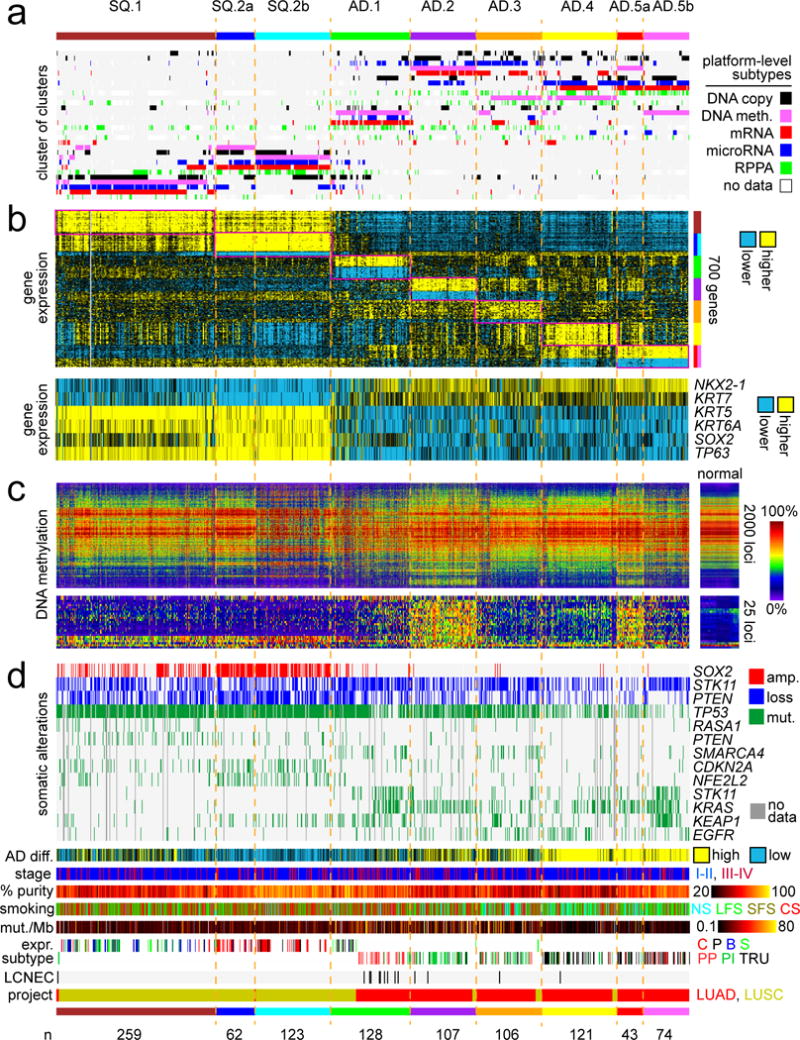
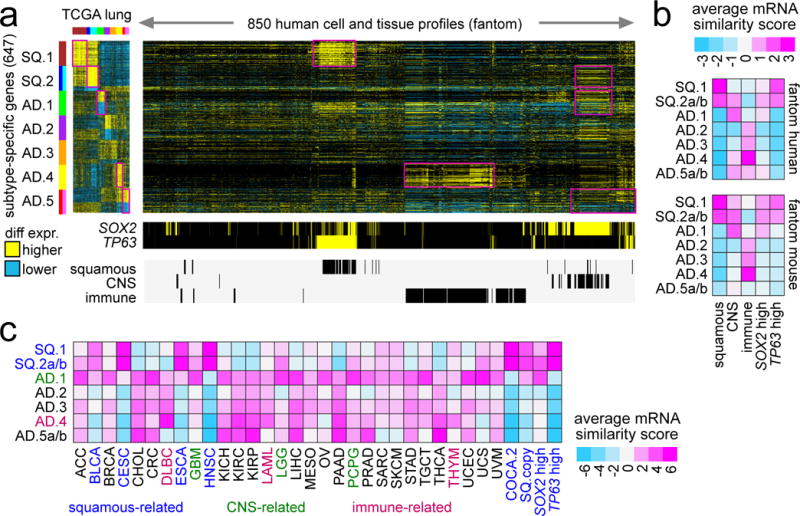
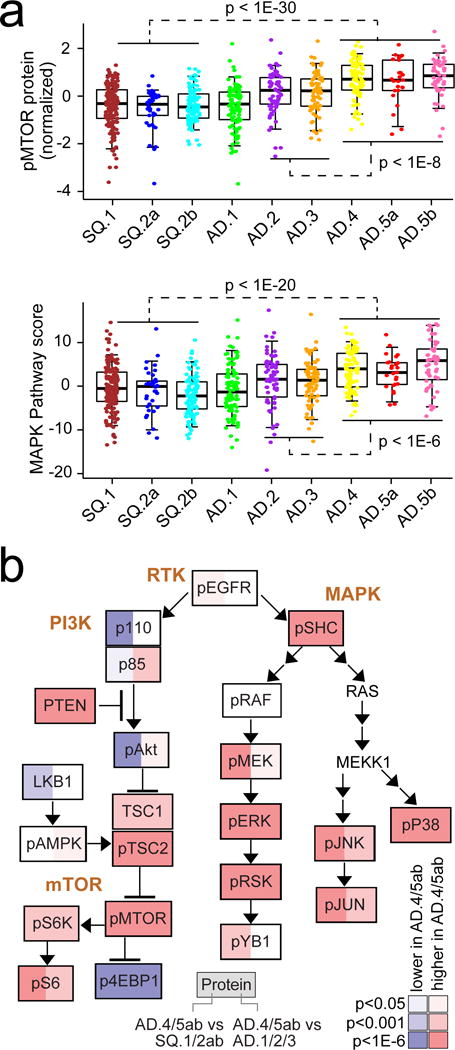
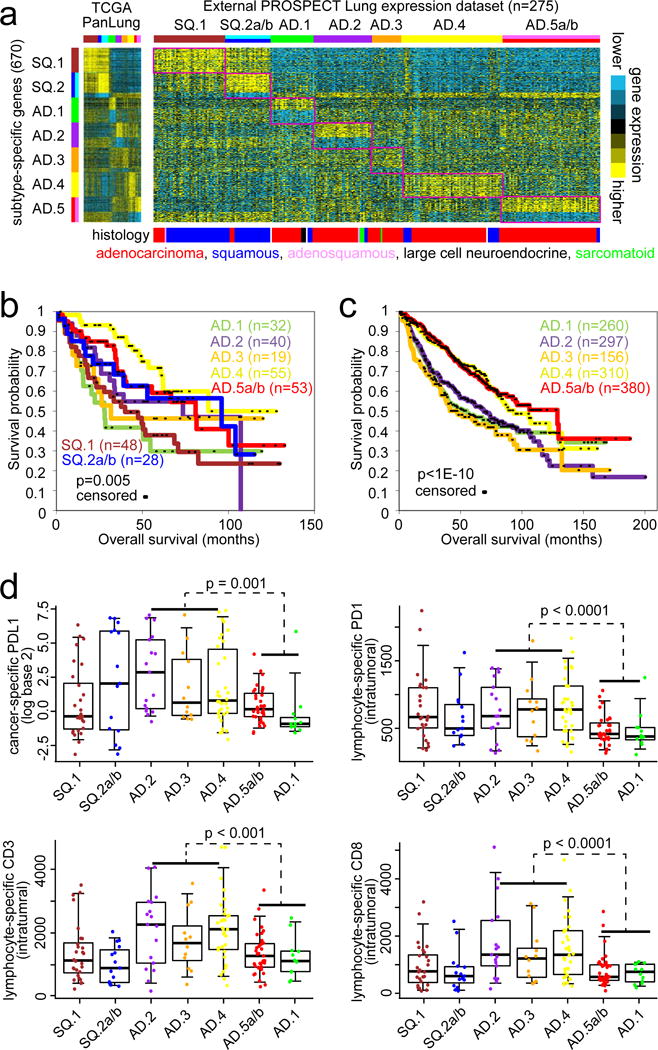
Non-small-cell lung cancer (NSCLC) demonstrates remarkable molecular diversity. With the completion of The Cancer Genome Atlas (TCGA), there is opportunity for systematic analyses of the entire TCGA NSCLC cohort, including comparisons and contrasts between different disease subsets. On the basis of multidimensional and comprehensive molecular characterization (including DNA methylation and copy, and RNA and protein expression), 1023 NSCLC cases-519 from TCGA adenocarcinoma (AD) project and 504 from TCGA squamous cell carcinoma (SQCC) project-were classified using a 'cluster-of-clusters' analytic approach. Patterns from TCGA NSCLC subsets were examined in independent external databases, including the PROSPECT (Profiling of Resistance patterns and Oncogenic Signaling Pathways in Evaluation of Cancers of the Thorax) NSCLC data set. Nine genomic subtypes of NSCLC were identified, three within SQCC and six within AD. SQCC subtypes were associated with transcriptional targets of SOX2 or p63. One predominately AD subtype (with a large proportion of SQCC) shared molecular features with neuroendocrine tumors. Two AD subtypes manifested a CpG island methylator phenotype. Three AD subtypes showed high p38 and mTOR pathway activation. AD subtypes associated with low differentiation showed relatively worse prognosis. SQCC subtypes and two of the AD subtypes expressed cancer testis antigen genes, whereas three AD subtypes expressed several immune checkpoint genes including PDL1 and PDL2, corresponding with patterns of greater immune cell infiltration. Subtype associations for several immune-related markers-including PD1, PDL1, CD3 and CD8-were confirmed in the PROSPECT cohort using immunohistochemistry. NSCLC molecular subtypes have therapeutic implications and lend support to a personalized approach to NSCLC management based on molecular characterization.
Conflict of interest statement
Figures

References
-
- Thomas A, Liu S, Subramaniam D, Giaccone G. Refining the treatment of NSCLC according to histological and molecular subtypes. Nat Rev Clin Oncol. 2015;12:511–526. - PubMed
-
- Beer DG, Kardia SL, Huang CC, Giordano TJ, Levin AM, Misek DE, et al. Gene-expression profiles predict survival of patients with lung adenocarcinoma. Nat Med. 2002;8:816–824. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
