

Incidence, Clinical Outcome and Risk Factors of Intensive Care Unit Infections in the Lagos University Teaching Hospital (LUTH), Lagos, Nigeria
- PMID: 27776162
- PMCID: PMC5077115
- DOI: 10.1371/journal.pone.0165242
Incidence, Clinical Outcome and Risk Factors of Intensive Care Unit Infections in the Lagos University Teaching Hospital (LUTH), Lagos, Nigeria
Abstract
Background: Infections are common complications in critically ill patients with associated significant morbidity and mortality.
Aim: This study determined the prevalence, risk factors, clinical outcome and microbiological profile of hospital-acquired infections in the intensive care unit of a Nigerian tertiary hospital.
Materials and methods: This was a prospective cohort study, patients were recruited and followed up between September 2011 and July 2012 until they were either discharged from the ICU or died. Antimicrobial susceptibility testing of isolates was done using CLSI guidelines.
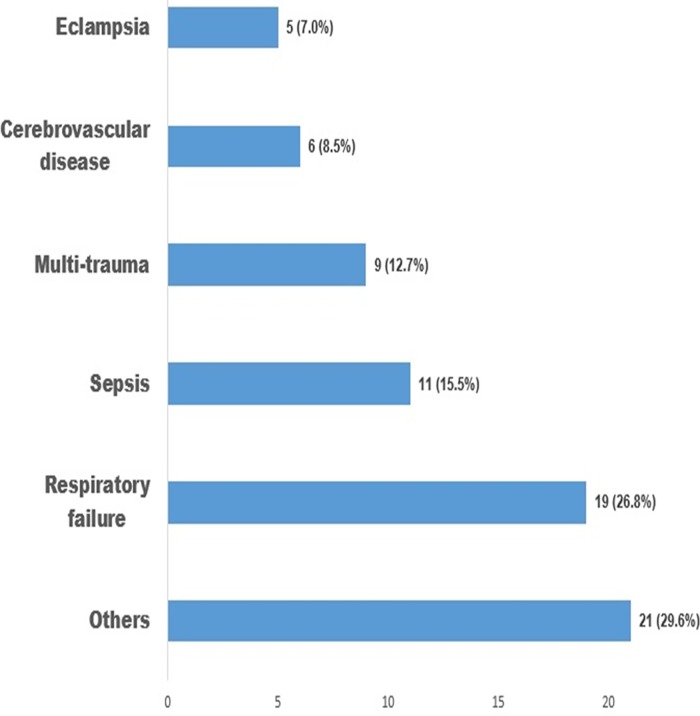
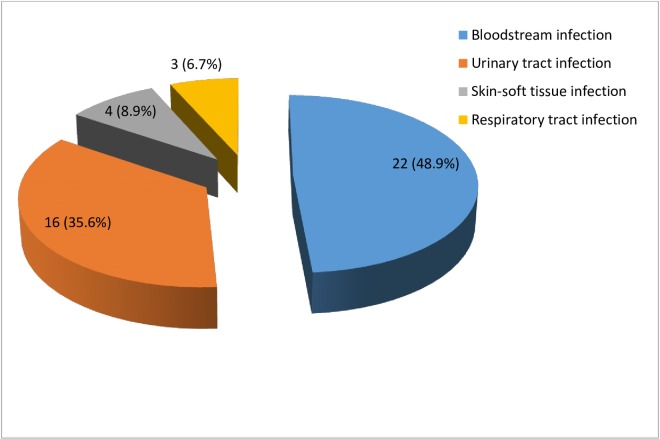
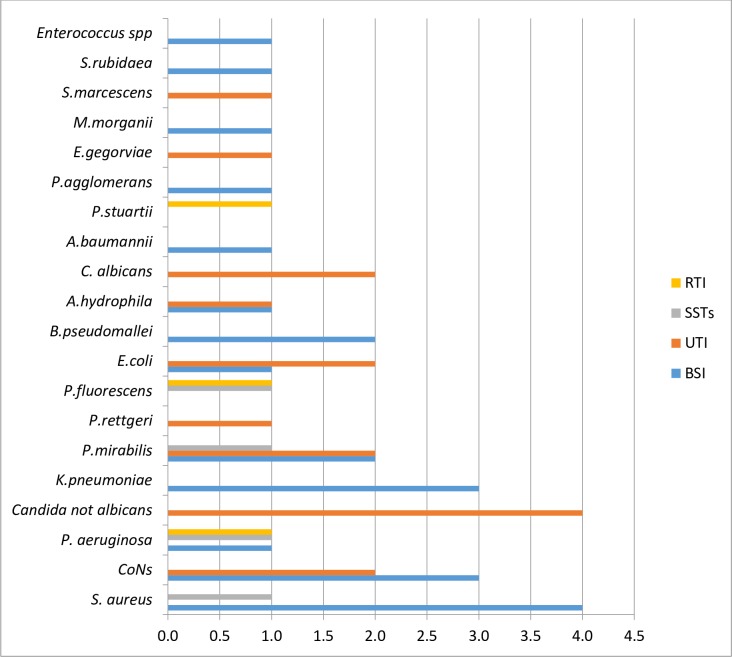
Results: Seventy-one patients were recruited with a 45% healthcare associated infection rate representing an incidence rate of 79/1000 patient-days in the intensive care unit. Bloodstream infections (BSI) 49.0% (22/71) and urinary tract infections (UTI) 35.6% (16/71) were the most common infections with incidence rates of 162.9/1000 patient-days and 161.6/1000 patient-days respectively. Staphylococcus aureus was the most common cause of BSIs, responsible for 18.2% of cases, while Candida spp. was the commonest cause of urinary tract infections, contributing 25.0% of cases. Eighty percent (8/10) of the Staphylococcus isolates were methicillin-resistant. Gram-negative multidrug bacteria accounted for 57.1% of organisms isolated though they were not ESBL-producing. Use of antibiotics (OR = 2.98; p = 0.03) and surgery (OR = 3.15, p< 0.05) in the month preceding ICU admission as well as urethral catheterization (OR = 5.38; p<0.05) and endotracheal intubation (OR = 5.78; p< 0.05) were risk factors for infection.
Conclusion: Our findings demonstrate that healthcare associated infections is a significant risk factor for ICU-mortality and morbidity even after adjusting for APACHE II score.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Tutuncu EE, Sencan I, Ozturk B, Senturk GC & Kilic AU. Device-associated infection rates and bacterial resistance in the intensive care units of a Turkish referral hospital. Saudi Medical Journal. 2011; 32(5):489–494. - PubMed
-
- World Health Organization. Health care-associated infections fact sheet. Available at: http://www.who.int/gpsc/country_work/gpsc_ccisc_fact_sheet_en.pdf, 2016
-
- Eugene I, Ikeh T, Erdoo S & Isamade T. Bacterial Flora of Fomites in a Nigerian Multi-Disciplinary Intensive Care Unit. Lab Medicine. 2011; 42: 411–413.
-
- Abubakar AS, Barma MM, Balla HJ, Tanimu YS, Waru GB, Dibal J. Spectrum of bacterial isolates among intensive care unit patients in a tertiary hospital in Northern Nigeria.Indian Journal of Scientific Research and Technology. 2014; 2(6):42–47
-
- Centre for Disease Prevention and Control (CDC). Guidelines for prevention of nosocomial pneumonia. Respiratory Care. 1994; 39:1191–1236. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
