

Neonatal bloodstream infections in a Ghanaian Tertiary Hospital: Are the current antibiotic recommendations adequate?
- PMID: 27776490
- PMCID: PMC5078915
- DOI: 10.1186/s12879-016-1913-4
Neonatal bloodstream infections in a Ghanaian Tertiary Hospital: Are the current antibiotic recommendations adequate?
Abstract
Background: Diagnosis of bloodstream infections (BSI) in neonates is usually difficult due to minimal symptoms at presentation; thus early empirical therapy guided by local antibiotic susceptibility profile is necessary to improve therapeutic outcomes.
Methods: A review of neonatal blood cultures submitted to the microbiology department of the Korle-Bu Teaching Hospital was conducted from January 2010 through December 2013. We assessed the prevalence of bacteria and fungi involved in BSI and the susceptibility coverage of recommended empiric antibiotics by Ghana Standard Treatment guidelines and the WHO recommendations for managing neonatal sepsis. The national and WHO treatment guidelines recommend either ampicillin plus gentamicin or ampicillin plus cefotaxime for empiric treatment of neonatal BSI. The WHO recommendations also include cloxacillin plus gentamicin. We described the resistance profile over a 28-day neonatal period using multivariable logistic regression analysis with linear or restricted cubic splines.
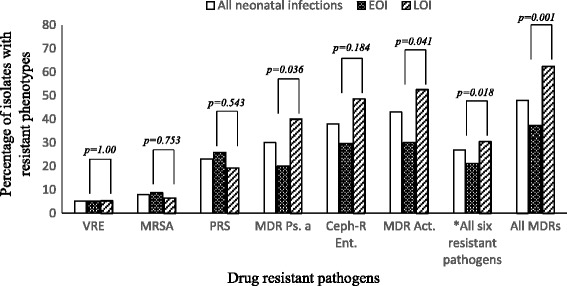
Results: A total of 8,025 neonatal blood culture reports were reviewed over the four-year period. Total blood culture positivity was 21.9 %. Gram positive organisms accounted for most positive cultures, with coagulase negative staphylococci (CoNS) being the most frequently isolated pathogen in early onset infections (EOS) (59.1 %) and late onset infections (LOS) (52.8 %). Susceptibility coverage of early onset bacterial isolates were 20.7 % to ampicillin plus cefotaxime, 32.2 % to the combination of ampicillin and gentamicin, and 71.7 % to cloxacillin plus gentamicin. For LOS, coverage was 24.6 % to ampicillin plus cefotaxime, 36.2 % to the combination ampicillin and gentamicin and 63.6 % to cloxacillin plus gentamicin. Cloxacillin plus gentamicin remained the most active regimen for EOS and LOS after exclusion of BSI caused by CoNS. For this regimen, the adjusted odds of resistance decreased between 12-34 % per day from birth to day 3 followed by the slowest rate of resistance increase, compared to the other antibiotic regimen, thereafter until day 28. The trend in resistance remained generally unchanged after excluding data from CoNS. Multidrug resistant isolates were significantly (p-value <0.001) higher in LOS (62.4 %, n = 555/886) than in EOS (37.3 %, n = 331/886).
Conclusions: There is low antibiotic susceptibility coverage for organisms causing neonatal bloodstream infections in Korle-Bu Teaching Hospital when the current national and WHO recommended empiric antibiotics were assessed. A continuous surveillance of neonatal BSI is required to guide hospital and national antibiotic treatment guidelines for neonatal sepsis.
Keywords: Antibiotics; Bloodstream; Ghana; Infections; Neonates; Resistance.
Figures


Similar articles
-
Trends in paediatric and adult bloodstream infections at a Ghanaian referral hospital: a retrospective study.Ann Clin Microbiol Antimicrob. 2016 Aug 18;15(1):49. doi: 10.1186/s12941-016-0163-z. Ann Clin Microbiol Antimicrob. 2016. PMID: 27539221 Free PMC article.
-
Early onset neonatal bloodstream infections in South African hospitals.BMC Infect Dis. 2025 Jan 20;25(1):85. doi: 10.1186/s12879-024-10406-z. BMC Infect Dis. 2025. PMID: 39833703 Free PMC article.
-
Susceptibility of bacterial etiological agents to commonly-used antimicrobial agents in children with sepsis at the Tamale Teaching Hospital.BMC Infect Dis. 2013 Feb 18;13:89. doi: 10.1186/1471-2334-13-89. BMC Infect Dis. 2013. PMID: 23419199 Free PMC article.
-
Literature review on the distribution characteristics and antimicrobial resistance of bacterial pathogens in neonatal sepsis.J Matern Fetal Neonatal Med. 2022 Mar;35(5):861-870. doi: 10.1080/14767058.2020.1732342. Epub 2020 Feb 26. J Matern Fetal Neonatal Med. 2022. PMID: 32102584 Review.
-
Evaluation of the Coverage of 3 Antibiotic Regimens for Neonatal Sepsis in the Hospital Setting Across Asian Countries.JAMA Netw Open. 2020 Feb 5;3(2):e1921124. doi: 10.1001/jamanetworkopen.2019.21124. JAMA Netw Open. 2020. PMID: 32049298 Free PMC article.
Cited by
-
Bacteriological Profile and Antibiotic Susceptibility Patterns of Sepsis-Causing Bacteria at the Neonatal Intensive Care Unit of a Tertiary Health Care Facility in Ghana.Microbiol Insights. 2023 Dec 11;16:11786361231218169. doi: 10.1177/11786361231218169. eCollection 2023. Microbiol Insights. 2023. PMID: 38090611 Free PMC article.
-
The Epidemiology of Bloodstream Infections and Antimicrobial Susceptibility Patterns: A Nine-Year Retrospective Study at St. Dominic Hospital, Akwatia, Ghana.J Trop Med. 2019 Sep 19;2019:6750864. doi: 10.1155/2019/6750864. eCollection 2019. J Trop Med. 2019. PMID: 31641359 Free PMC article.
-
Microbial Distribution and Antibiotic Susceptibility of Bloodstream Infections in Different Intensive Care Units.Front Microbiol. 2021 Dec 9;12:792282. doi: 10.3389/fmicb.2021.792282. eCollection 2021. Front Microbiol. 2021. PMID: 34956159 Free PMC article.
-
Prevalence of carbapenem-resistant and extended-spectrum beta-lactamase-producing Enterobacteriaceae in a teaching hospital in Ghana.PLoS One. 2023 Oct 30;18(10):e0274156. doi: 10.1371/journal.pone.0274156. eCollection 2023. PLoS One. 2023. PMID: 37903118 Free PMC article.
-
Surveillance for incidence and etiology of early-onset neonatal sepsis in Soweto, South Africa.PLoS One. 2019 Apr 10;14(4):e0214077. doi: 10.1371/journal.pone.0214077. eCollection 2019. PLoS One. 2019. PMID: 30970036 Free PMC article.
References
-
- Muller-Pebody B, Johnson AP, Heath PT, Gilbert RE, Henderson KL, Sharland M, iCAP Group (Improving Antibiotic Prescribing in Primary Care) Empirical treatment of neonatal sepsis: are the current guidelines adequate? Arch Dis Child - Fetal Neonatal Ed. 2011;96:F4–F8. doi: 10.1136/adc.2009.178483. - DOI - PubMed
-
- Enweronu-Laryea CC, Newman MJ. Changing pattern of bacterial isolates and antimicrobial susceptibility in neonatal infections in Korle-Bu Teaching hospital, Ghana. East Afr Med J. 2007;84:164–167. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
